BURNOUT · PART 4
The Anatomy of Neurodivergent Burnout — Part 4: Recovery
Clinical protocols for recovering from neurodivergent burnout: polyvagal theory, the four phases of recovery, and practical strategies.
Introduction: Recovery Is Not a Return
The first thing you need to hear is this: recovery from neurodivergent burnout does not mean going back to "normal." That "normal" is what brought you here. That "normal" was a mask worn so long you confused it with your face. That "normal" was a nervous system running at 100% without breaks, without accommodations, without permission to be what you are.
Authentic recovery means something else entirely: building, perhaps for the first time, a life that respects your neurology. Not one where you "function" — one where you actually live.
Research confirms this: recovery from autistic burnout requires not just reducing demands but a fundamental reconfiguration of the relationship with one's own self (Raymaker et al., 2020). Study participants describe recovery not as a return to the prior state but as a rediscovery: "I learned who I actually am, not who I was pretending to be" (Higgins et al., 2021).
This process is not linear. It is not fast. And it is not something you can power through with willpower alone. But it is possible. And it begins with understanding what is happening in your nervous system.
◆ ◆ ◆
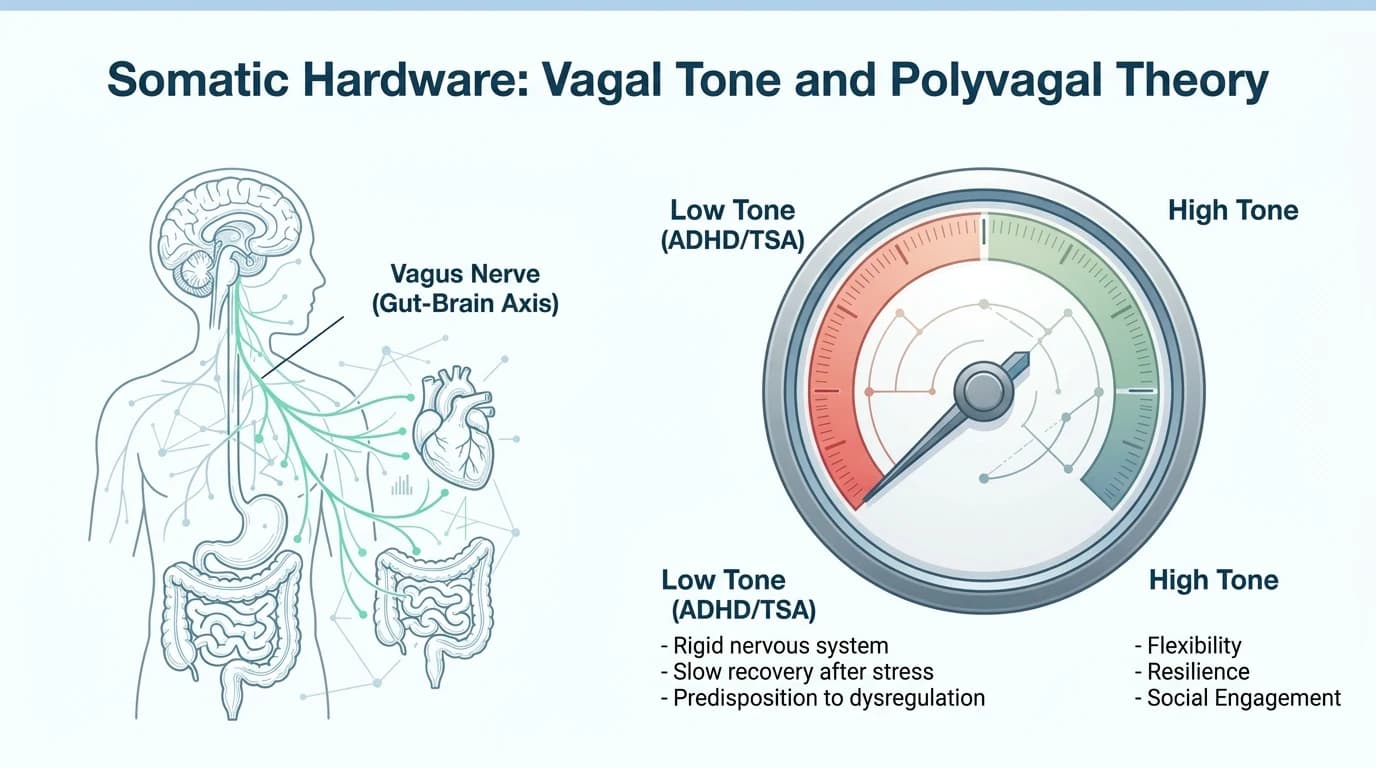
Polyvagal Theory and the Nervous System in Burnout
The three states of the autonomic nervous system
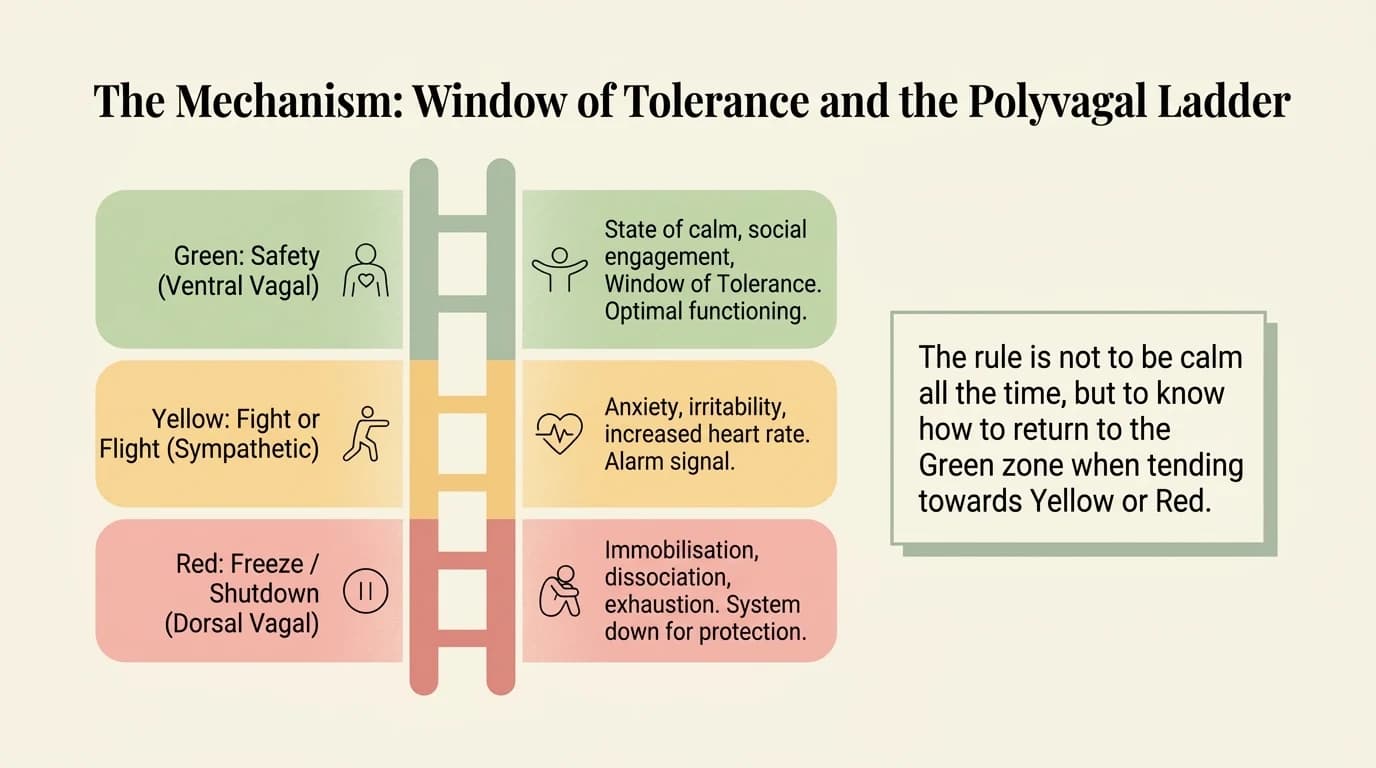
Stephen Porges (2011) described the autonomic nervous system not as a simple switch (on/off) but as a ladder with three rungs:
- Ventral vagal (safety and connection) — the state where you can think clearly, connect with others, process emotions. The body is relaxed yet alert. This is where creativity, intimacy, and play live.
- Sympathetic (fight or flight) — the mobilization state. Heart rate rises, muscles tense, attention narrows. Useful in genuine danger. Devastating when it becomes chronic — and for a neurodivergent nervous system in a neurotypical environment, it often becomes the default.
- Dorsal vagal (collapse, shutdown) — the state of extreme conservation. The body shuts down. Zero energy. Dissociation. The inability to speak, think, or act. This is the state of deep burnout.
Burnout as dorsal vagal lockout
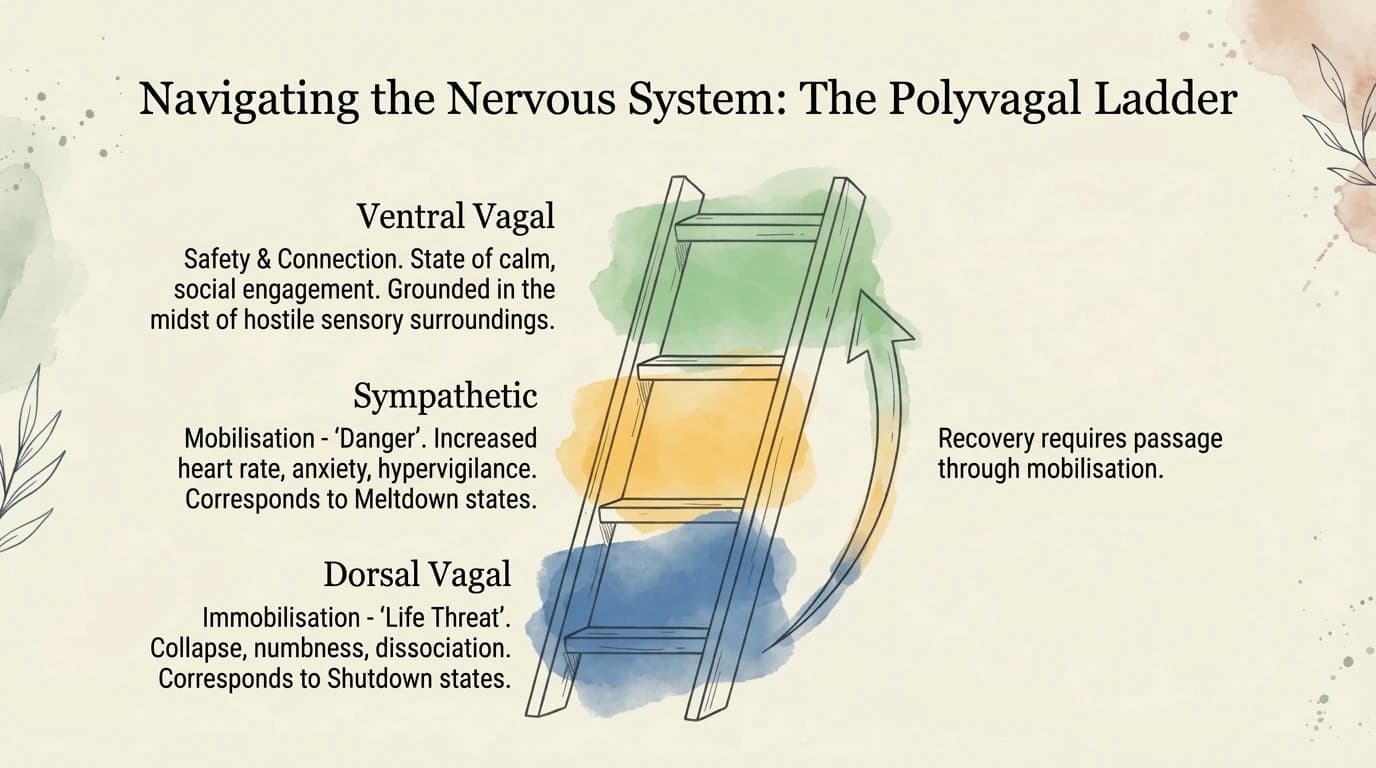
Deb Dana (2020) extended Porges's work into direct clinical applications. What she describes as "dorsal collapse" is precisely what neurodivergent people describe in burnout: unable to speak, unable to think, unable to get out of bed. It is not laziness. It is not depression. It is a nervous system that has crossed the overload threshold and entered energy conservation mode — the neurophysiological equivalent of a circuit breaker disconnecting to prevent a fire.
The clinical implication is profound: you cannot think your way out of dorsal vagal collapse. Higher cognitive functions — planning, motivation, reasoning — are offline. The way out runs through the body, not the mind. Through sensory safety, co-regulation, micro-movements that signal the vagus nerve that the danger has passed.
Neuroception: Why your body doesn't believe you when you say "I'm safe"
Porges (2011) introduced the concept of "neuroception" — the unconscious, automatic assessment the nervous system makes continuously: am I safe or in danger? This evaluation does not pass through the prefrontal cortex. It does not account for logic. It operates subcortically, relying on sensory signals: someone's vocal tone, the light in the room, the sounds around you, the texture of your chair.
For neurodivergent people, neuroception is often recalibrated by experience: after years of hostile environments, invalidation, and forced masking, the nervous system has learned that the world is not safe. And it continues operating on that premise even in objectively safe settings. This is one of recovery's greatest challenges: it is not enough to be safe — your nervous system must believe you are safe.
◆ ◆ ◆
Clinical Protocols Adapted for Neurodivergent Recovery
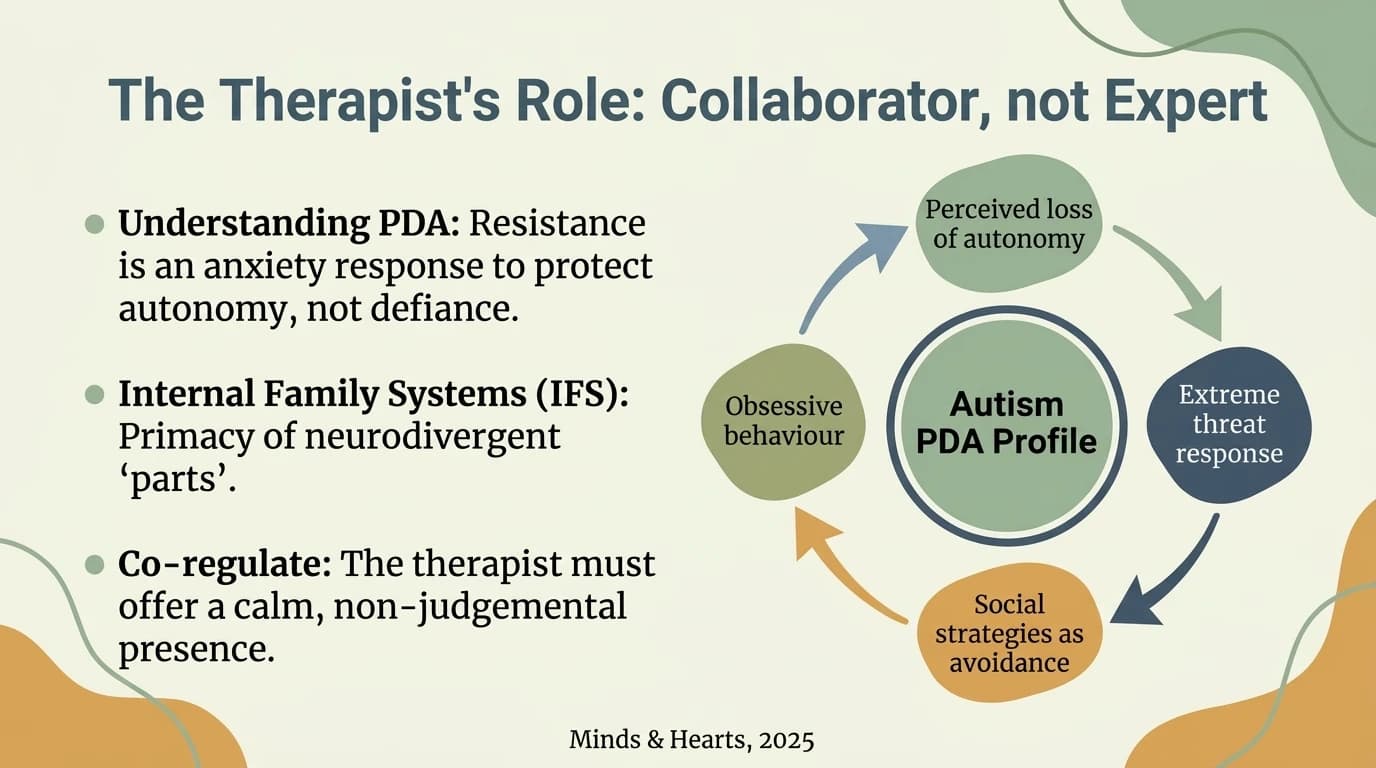
IFS (Internal Family Systems): Working with parts
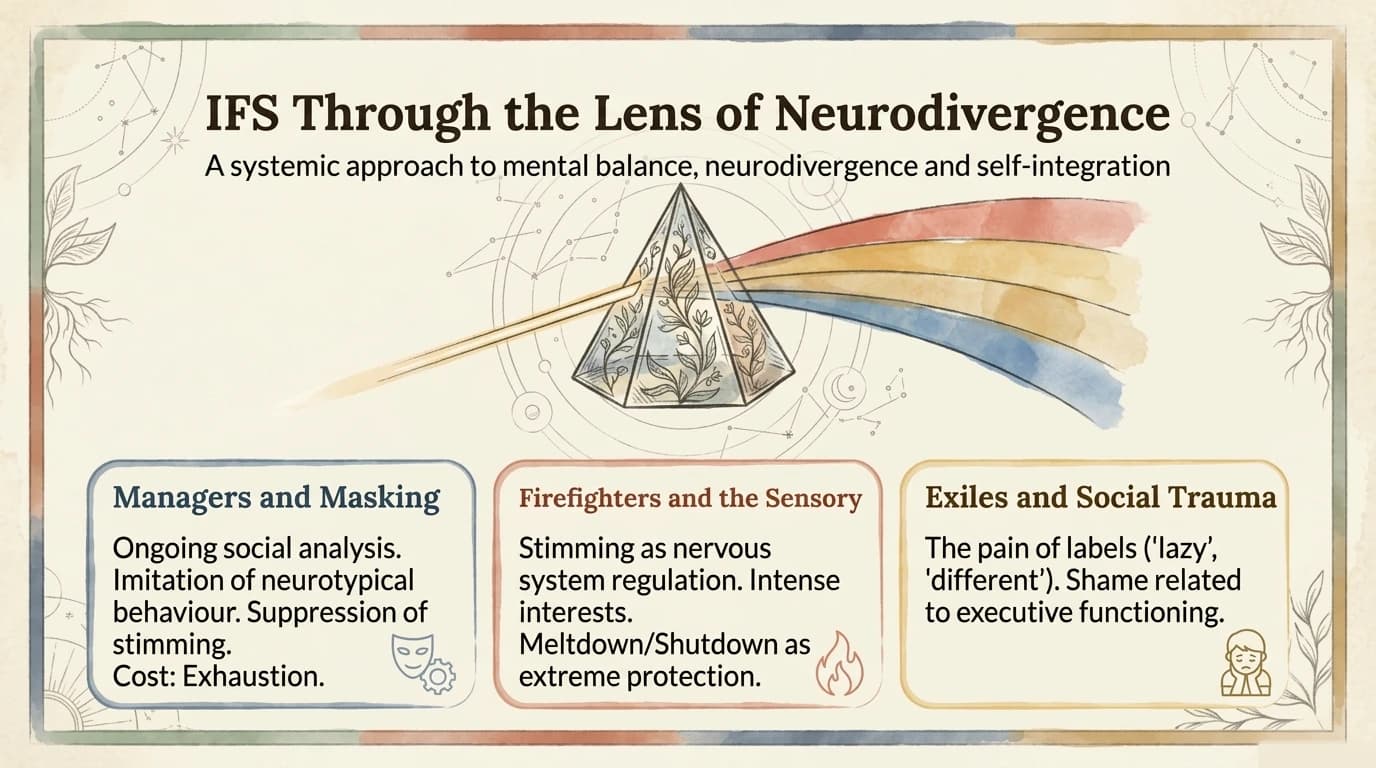
Richard Schwartz developed a therapeutic model that treats the mind as a system of "parts" — each with its own function, its own story, its own protective intention. For neurodivergent people, IFS is particularly relevant:
The masking part is not the enemy. It is a protector that learned, correctly, that authenticity gets punished. Recovery does not mean eliminating it but acknowledging the role it played and renegotiating the terms. "Thank you for protecting me. You don't have to do this all the time anymore."
The collapsing part is not weakness. It is an internal firefighter pulling the emergency brake. Instead of fighting the collapse, IFS proposes curiosity: what is this part trying to protect? What happens if you listen to it rather than force it to disappear?
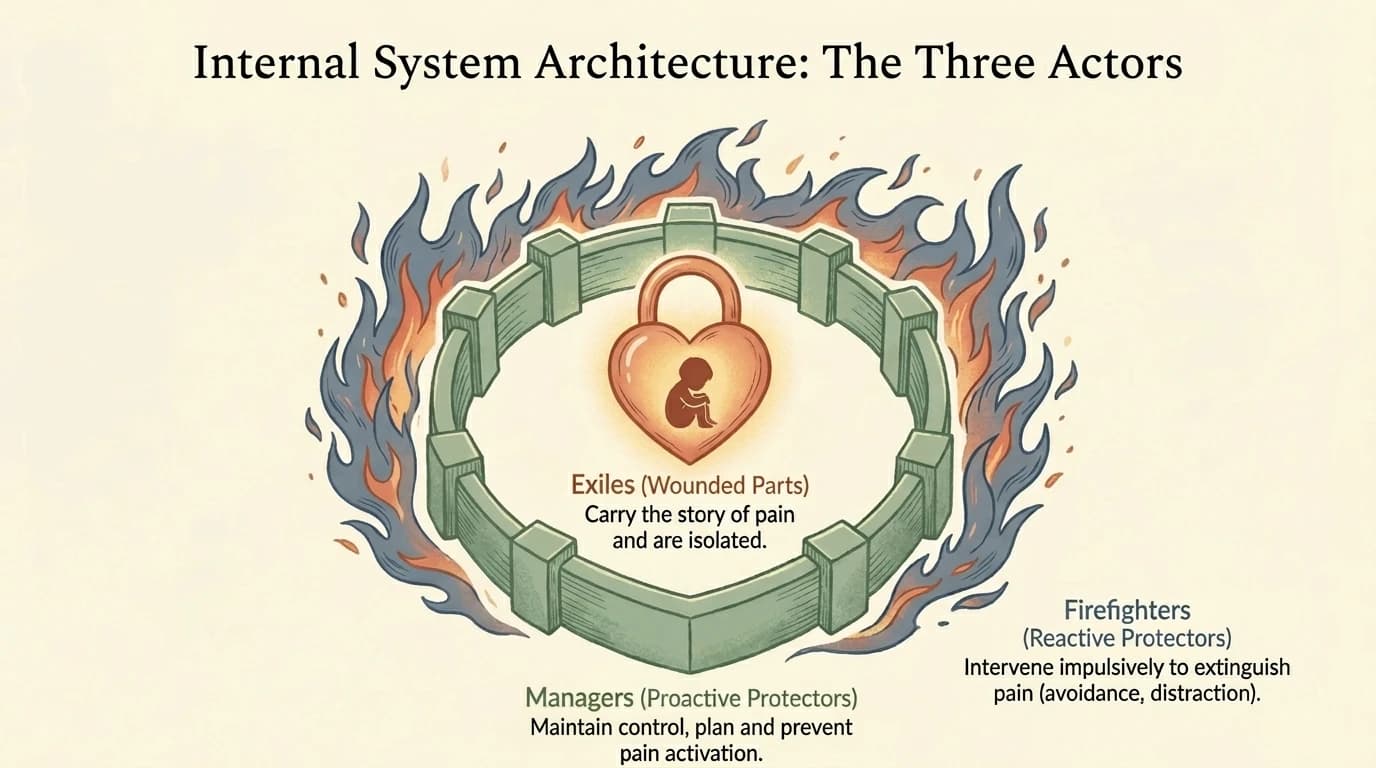
Preliminary research suggests IFS holds promise for neurodivergent populations precisely because it does not pathologise survival mechanisms but respects them as intelligent responses to hostile environments (Anderson et al., 2017).
IFS adaptations for neurodivergent clients: Traditional IFS relies on internal visualization — a real challenge for people with aphantasia or predominantly analytical thinking styles. Neuro-affirmative practice uses Tactile IFS: stones, figurines, or sandtrays as external representations of parts, allowing work with the internal system through concrete sensory channels. For clients with analytical cognitive styles, mapping parts on paper or a digital board — with arrows, colors, and labels — can be more accessible than classical guided introspection. Additionally, in IFS work with autistic individuals, it is essential to differentiate neurology from protective parts: difficulty maintaining eye contact is not a "part" requiring therapeutic work — it is simply how that brain operates (Schwartz & Sweezy, 2020).
Somatic approaches: The body as gateway
When the prefrontal cortex is offline — in deep burnout — cognitive approaches cannot reach where they need to go. Somatic approaches work directly with the body:
Somatic Experiencing (Peter Levine) — based on the observation that wild animals process traumatic experiences through involuntary body trembling. Humans suppress this process. SE helps the nervous system complete activation cycles that remained "stuck" — releasing energy stored in the body (Levine, 2010).
Orienting exercises — simple head and eye movements that scan the environment, communicating to the vagus nerve: "I am here. It is safe." Deb Dana (2020) recommends this as a starting point for people in dorsal collapse: slowly move the head from left to right, observing objects in the room, naming them mentally.
Stimming as somatic regulation — what pathology calls "repetitive behaviour" is, from a neuro-affirmative perspective, a nervous system self-regulation mechanism (Kapp et al., 2019). Rocking, humming, repeatedly touching a texture — all are forms of vestibular, proprioceptive, or tactile stimulation that help return to the window of tolerance. In recovery, stimming should not be suppressed. It should be encouraged.
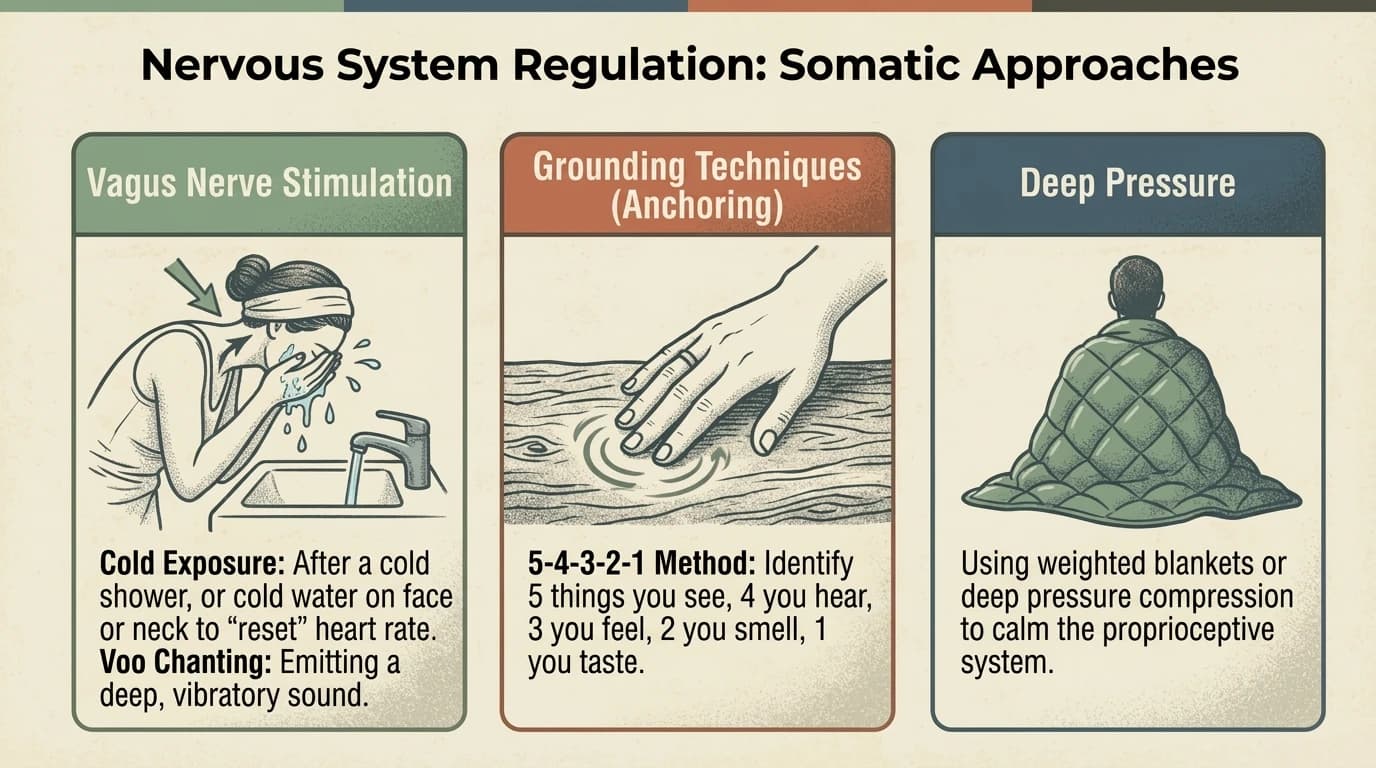
Specific vagal tone exercises: The vagus nerve can be directly stimulated through simple techniques with measurable effects on heart rate variability (Porges, 2011; Dana, 2020):
- Cold exposure: Submerging the face in cold water (10-15°C) for 15-30 seconds activates the dive reflex and stimulates the ventral branch of the vagus nerve. Alternatively, a 30-second cold rinse at the end of a warm shower.
- Extended vocalization: Humming, singing, or sustained pronunciation of the sound "voo" (recommended by Peter Levine) physically vibrates the vagus nerve through the larynx. 2-3 minutes of vocalization produces a measurable drop in heart rate.
- Extended-exhale breathing: Inhale 4 seconds, exhale 8 seconds — the 1:2 ratio activates the parasympathetic branch. The most accessible vagal exercise, it can be practiced discreetly in any context.
Sensory-adapted DBT
Dialectical Behavior Therapy (Linehan, 1993) offers concrete emotional regulation tools. Adapted for neurodivergent needs (Strang & Sakdalan, 2025), DBT becomes less verbal and more sensory:
- TIPP (Temperature, Intense Exercise, Paced Breathing, Paired Muscle Relaxation) — crisis interventions that work directly with the autonomic nervous system
- Distress tolerance through controlled sensory stimulation: ice on wrists, weighted blanket, rhythmic sound
- Adapted mindfulness — not classical meditation (which can be dissociative for alexithymic individuals), but concrete sensory awareness: "What are you touching right now? What do you hear? What do you see?"
◆ ◆ ◆
The Four Phases of Recovery
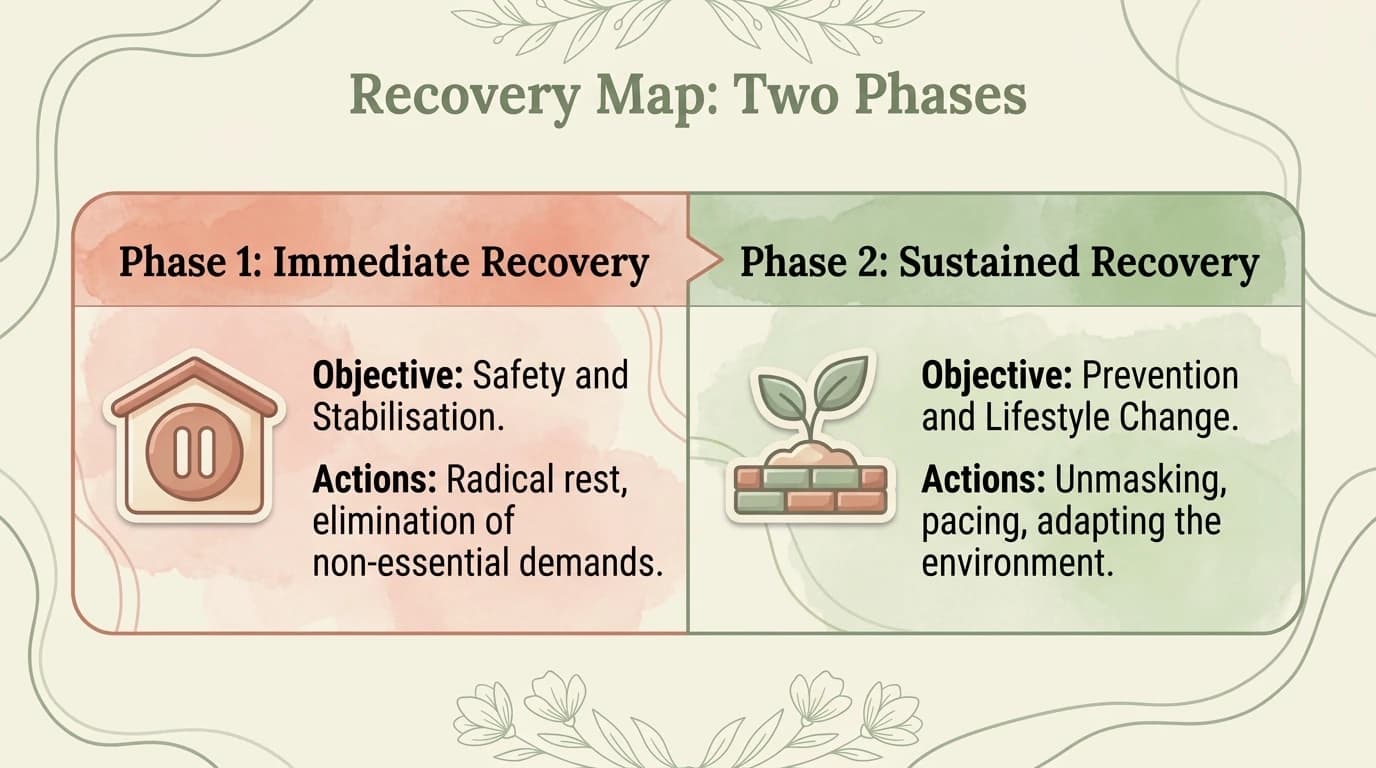
Recovery from neurodivergent burnout is not an event — it is a process that unfolds in phases. Forcing yourself to skip phases does not accelerate recovery; it sabotages it.
Phase 1: Collapse and withdrawal
What happens: The nervous system has given out. The ability to function drops dramatically — verbally, cognitively, executively, socially. This is not a choice. It is a neurophysiological shutdown.
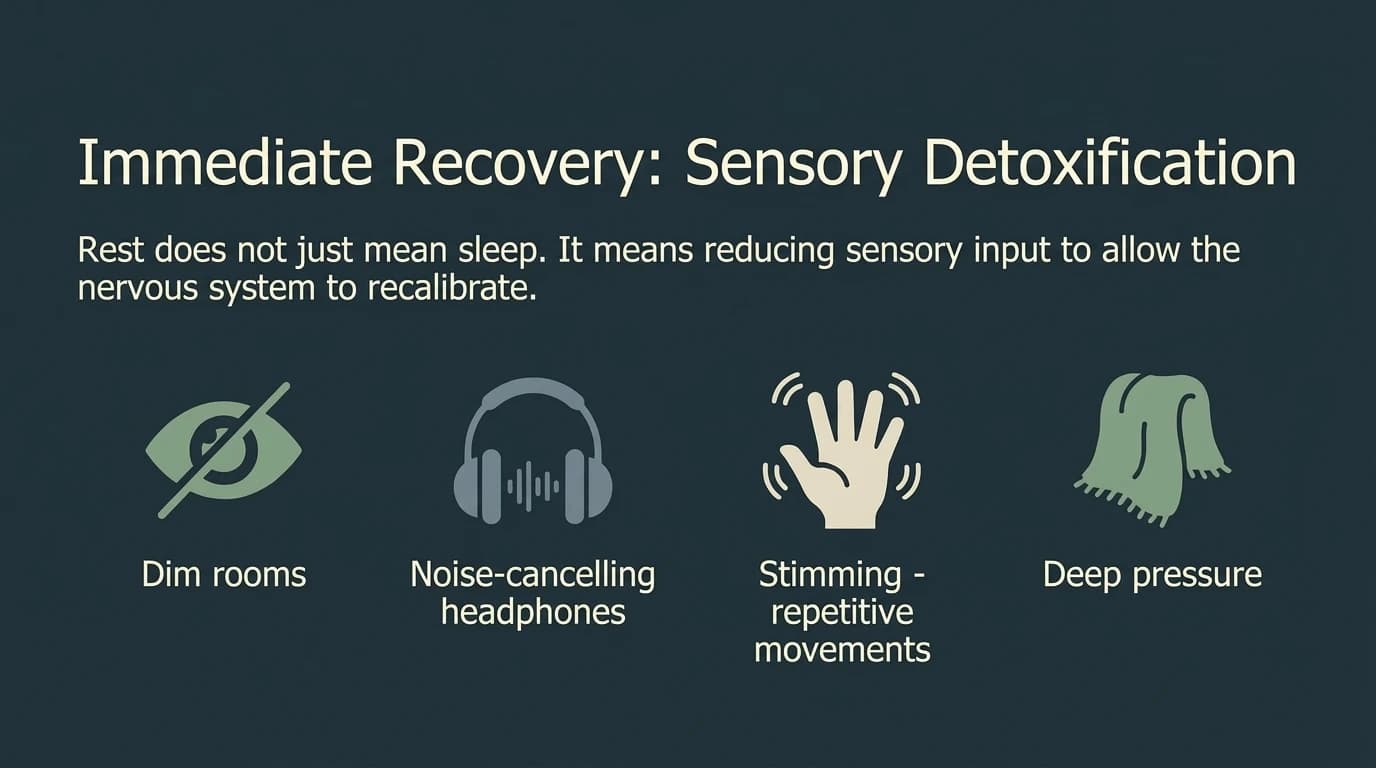
What you need: Complete withdrawal. Demands reduced to the vital minimum. Radical rest — not "active rest" (reading, light socializing, hobbies). Real rest: silence, darkness, the absence of any demand. Stimming permitted without restriction. Zero pressure to "be productive" or to "work on recovery."
How long: Weeks or months. There is no shortcut. Any external or self-imposed pressure to "come back" extends this phase.
Phase 2: Stabilization
What happens: The first signs of return. Not consistent energy, but moments of energy followed by periods of fatigue. Executive functions appear intermittently. Special interests may begin to return — this is one of the most reliable signs of stabilization.
What you need: Minimal, predictable routine with no surprises. Daily energy accounting (what you have, not what you wish you had). Interoception micro-exercises (Mahler, 2024). Reconnection with the body through preferred sensory stimulation. Co-regulation with 1-2 safe people.
The major risk: The "false window" phase — a period of apparent energy that tempts a return to the previous pace. This is a trap. The body is testing, not confirming. If you overload now, you return to Phase 1.
The false window is particularly dangerous for people with ADHD, where impulsivity and energetic optimism can turn one good day into massive overexertion. Signs you're in a false window, not real recovery: energy appears suddenly (not gradually), you feel an urgent need to "make up for lost time," and the absence of fatigue seems suspiciously complete. The golden rule: after the first "normal" day, wait three more days at the same level before adding new activities (Raymaker et al., 2020).
Phase 3: Gentle re-engagement
What happens: Energy becomes more stable. You can begin adding activities — one at a time, gradually, with monitoring. You do not return to the previous schedule. You build a new one, based on what you have learned about your real capacities.
What you need: The two-thirds principle — plan to do two-thirds of what you think you can manage (Raymaker et al., 2020). Rigorous pacing. Transition time between activities. Daily assessment: "Is today green, yellow, or red?" (the traffic light system). Reintroduce masking only strategically, not automatically — and only with planned recovery afterward.
Phase 4: Rebuilding and recalibration
What happens: Not "returning to normal," but building a new normal. This is the moment where you integrate everything you have learned: what depletes you, what recharges you, what is negotiable and what is not.
What you need: Environmental redesign (home, work, relationships). Permanent accommodations, not temporary ones. A prevention plan for the future. Rebuilt identity — who you are without the mask, not who you were with it. Ongoing neuro-affirmative therapy.
◆ ◆ ◆
Co-Regulation and Safe Relationships
Why you cannot do this alone
Polyvagal theory shows us that the human nervous system was not designed for isolated self-regulation. It was designed for co-regulation — the presence of another nervous system that communicates safety (Porges, 2011). The tone of voice, the rhythm of breathing, the facial expression of the person beside you — all are signals that the vagus nerve interprets before you are consciously aware of them.
In burnout, the capacity for self-regulation is compromised. Co-regulation becomes not a luxury — but a biological necessity.
"Anchor people"
You do not need many people. You need 2-3 who meet certain conditions (Price, 2022; Dana, 2020):
- Their presence reduces, not increases, your nervous system activation
- They do not demand social performance — you can be silent, you can stim, you can exist unmasked
- They communicate safety through presence, not words — a calm nervous system beside yours is more powerful than any advice
- They do not try to "fix" — they listen, validate, sit beside you
Inter-autistic resonance
Crompton et al. (2020) demonstrated that information transfer between autistic people is as effective as between neurotypical people — and significantly more effective than between a neurotypical and an autistic person. This is not merely a communication finding. It is a co-regulation finding: with other neurodivergent people, the cost of masking disappears completely. You can simply exist. Nothing more. And that, in itself, is therapeutic.
Neurodivergent communities — physical or online — function as co-regulation spaces where the nervous system can rest from the perpetual translation effort.
◆ ◆ ◆
Practical Recovery Strategies
Sensory diet
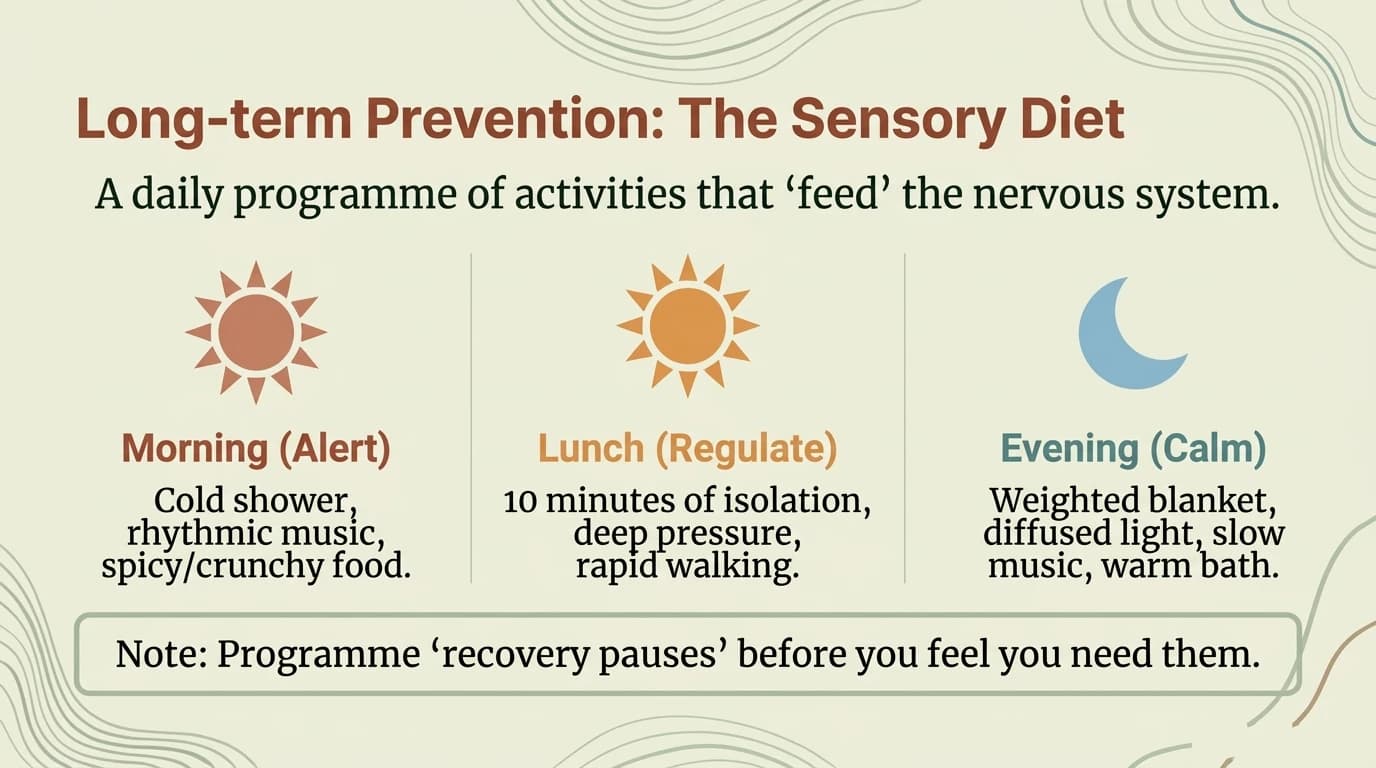
Just as you have a food diet, you can build a "sensory diet" — a deliberate plan of sensory stimulation and protection tailored to your needs (Wilbarger & Wilbarger, 2002):
- Proprioceptive input (deep pressure): weighted blanket, firm hugs, isometric exercises — calms the activated nervous system
- Vestibular input (rhythmic movement): swinging, rocking, walking — regulates the dorsal vagal nervous system
- Auditory protection: noise-canceling headphones, white noise, familiar ambient music
- Visual protection: dimmable lights (2700K), blue light filter glasses, standby LED covers
- Preferred tactile input: familiar textures, fidget objects, tagless clothing
Energy accounting
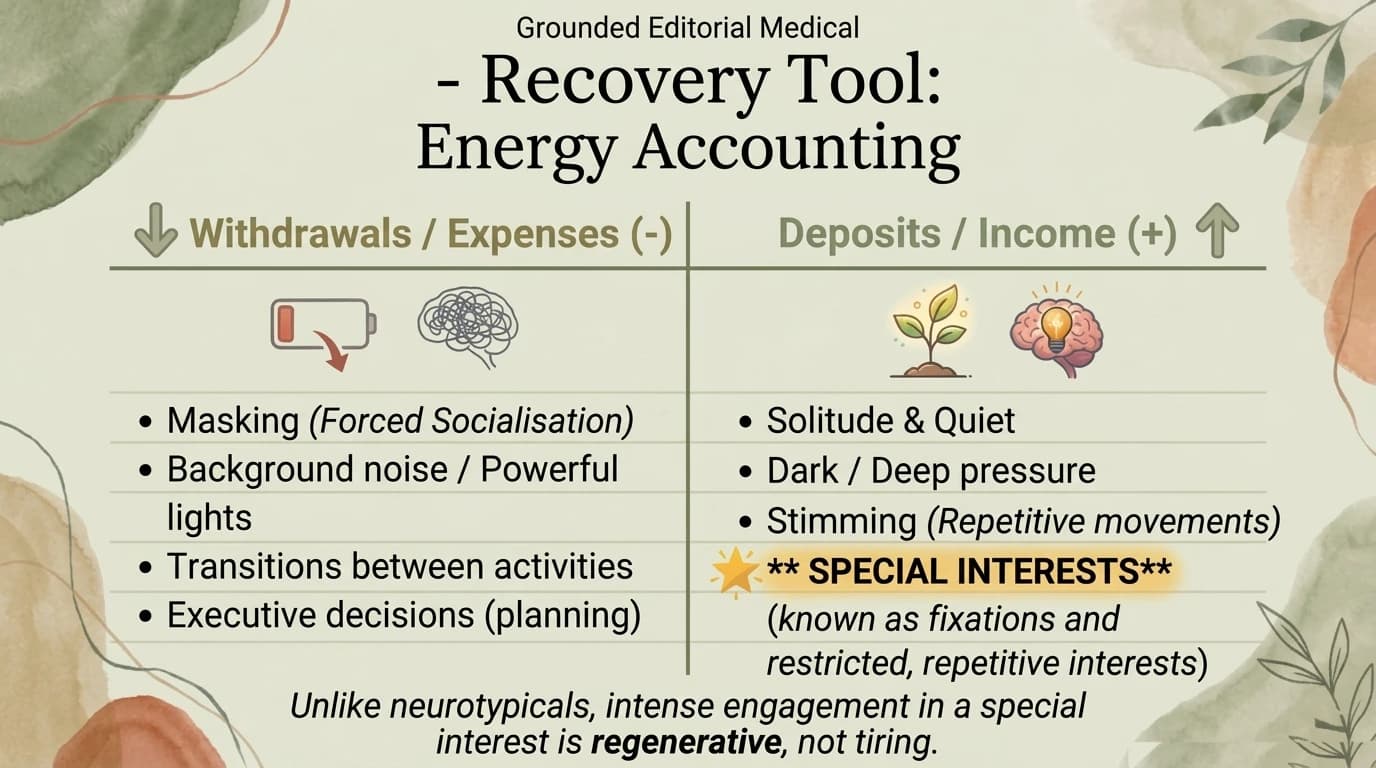
Adapted from the Maja Toudal framework (Neurodivergent Insights, 2023): each morning, assess the four energy types (body, brain, emotional, masking) on a 0-10 scale. Plan your day based on what you have, not what you wish you had. If masking energy is 2/10, today is not the day for meetings with strangers.
Rest without guilt
This may be the hardest strategy to implement, because internalized ableism constantly whispers: "You're not doing enough. Others manage. You're just lazy."
Rest is not a reward for productivity. It is a biological necessity. A neurodivergent nervous system in recovery needs more rest than before burnout — not less. And "rest" does not mean "a less demanding activity." It means the absence of any demand. It means permission to exist without producing.
Special interests as healing tools
Special interests are not "obsessions." They are sources of dopamine, flow, and authentic joy. The return of special interests is one of the most reliable indicators of recovery (Higgins et al., 2021). Do not force them. But when they return — even as brief sparks — follow them. They are the nervous system signaling: I am beginning to have energy for things that matter.
◆ ◆ ◆
When You Need Professional Help
Neuro-affirmative therapy
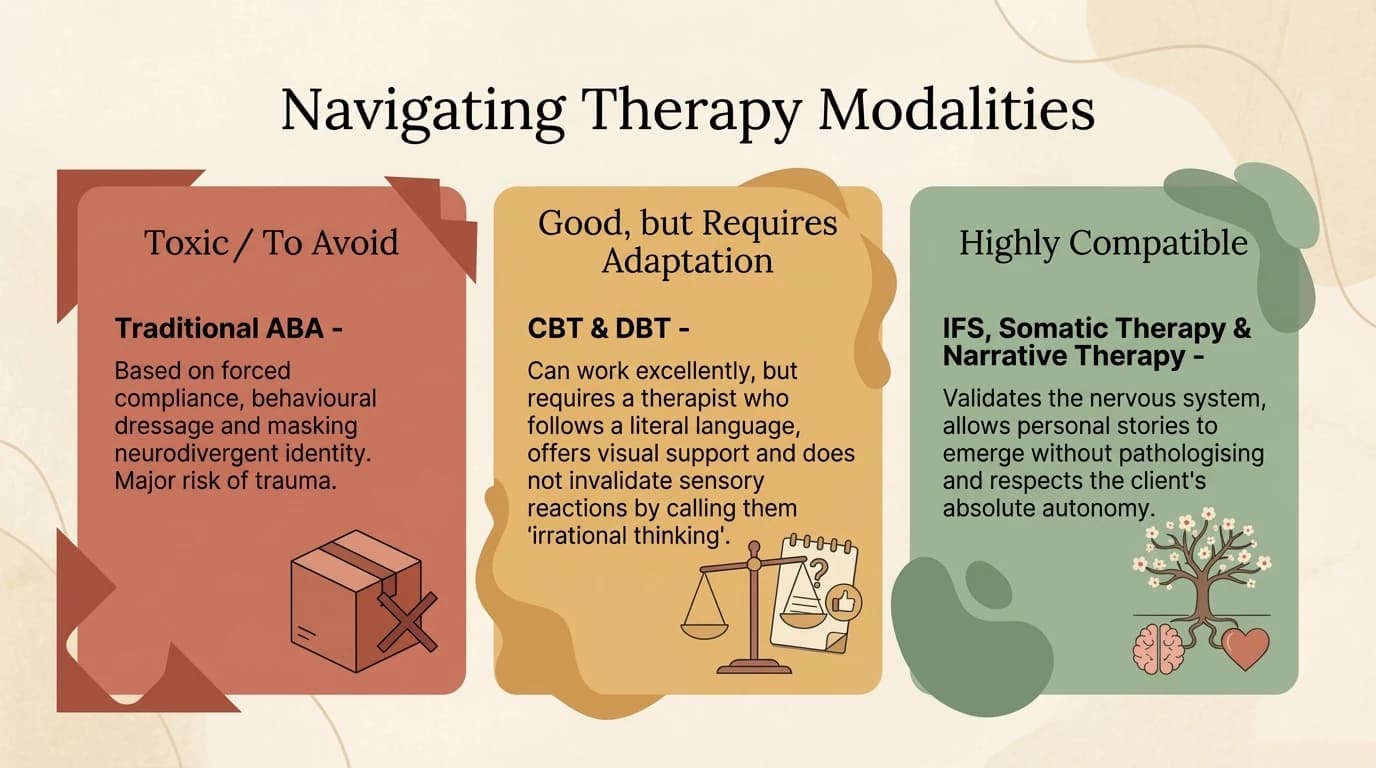
Not every therapist can work with neurodivergent burnout. A neuro-affirmative therapist (Pahnke et al., 2023):
- Understands the difference between autistic burnout and clinical depression
- Does not recommend behavioral activation during burnout (which worsens collapse)
- Uses evidence-based approaches adapted for ND populations: ACT, IFS, SE, sensory DBT
- Accepts atypical communication: long pauses, non-verbalization, written communication, avoiding eye contact
- Views masking as a survival mechanism, not a "social skill to maintain"
- Works with the nervous system, not against it
Medication considerations
Medication does not treat neurodivergent burnout — there is no pill for systemic exhaustion. But it can address comorbidities that complicate recovery:
- Chronic anxiety that prevents ventral vagal activation
- Insomnia that sabotages physiological restoration
- Untreated ADHD where stimulant medication can reduce executive burden
- Comorbid depression (not burnout misdiagnosed as depression, but depression alongside burnout) Any medication decision should be made with a psychiatrist who understands neurodivergence — not one who will prescribe SSRIs for what is actually autistic exhaustion.
Emergency signals
Neurodivergent burnout correlates with suicidal ideation in approximately 44% of those affected (Pelton & Cassidy, 2017; Cassidy et al., 2018). If you find yourself in any of these descriptions, do not delay:
- Persistent thoughts that "it would be better without me"
- Complete loss of the ability to function for more than 2 weeks
- Total isolation — not just withdrawal, but the complete absence of any contact
- Self-harm or self-destructive behaviours Seeking help is not weakness. It is, in itself, an act of recovery.
◆ ◆ ◆
What Comes Next in Part 5
Over four articles, we have covered the complete anatomy of neurodivergent burnout: what it is (Part 1), the invisible mechanisms (Part 2), the external factors (Part 3), and now — the road to recovery (Part 4).
But recovery without prevention is a cycle. In Part 5 — "Prevention and Sustainability" — we close the circle:
- The early warning system — detecting burnout before collapse
- Energy Accounting — daily energy management
- Architecting a sustainable life — redesigning the environment, not adapting yourself
- Masking budget — when, how much, and how to reduce
- Safety nets — what to have prepared before crisis
- Long-term monitoring — how not to forget you are vulnerable Recovery teaches you to get up. Prevention teaches you to stop falling.
Ready to take the next step?
If what you have read resonates with you, you are not alone. Neurodivergent burnout is a real, research-validated experience — and there are neuroaffirmative strategies that can help.
Schedule an Initial Consultation →
Resources and support:
National Suicide Prevention Lifeline (US): 988 (call or text, 24/7)
Crisis Text Line: text HOME to 741741
Samaritans (UK): 116 123 (24/7)
Autism Society: autismsociety.org
CHADD (ADHD): chadd.org
References
- Anderson, F. G., Sweezy, M., & Schwartz, R. C. (2017). Internal Family Systems Skills Training Manual. PESI Publishing.
- Cassidy, S., et al. (2018). Risk markers for suicidality in autistic adults. Molecular Autism, 9(1), 42.
- Crompton, C. J., et al. (2020). Autistic peer-to-peer information transfer is highly effective. Autism, 24(7), 1704-1712.
- Dana, D. (2020). Polyvagal Exercises for Safety and Connection. W. W. Norton.
- Higgins, J. M., et al. (2021). Defining autistic burnout through experts by lived experience. Autism, 25(8), 2356-2369.
- Kapp, S. K., et al. (2019). Autistic adults' views and experiences of stimming. Autism, 23(7), 1782-1792.
- Levine, P. A. (2010). In an Unspoken Voice. North Atlantic Books.
- Linehan, M. M. (1993). Cognitive-Behavioral Treatment of Borderline Personality Disorder. Guilford Press.
- Mahler, K. (2024). 30 Days of Interoception Activities. Kelly Mahler OTD.
- Neurodivergent Insights / Toudal, M. (2023). Energy Accounting Worksheets. neurodivergentinsights.com
- Pahnke, J., et al. (2023). ACT for autistic adults: RCT. Autism (SAGE).
- Pelton, M. K., & Cassidy, S. A. (2017). Are autistic traits associated with suicidality? Autism Research, 10(10), 1643-1662.
- Porges, S. W. (2011). The Polyvagal Theory. W. W. Norton.
- Price, D. (2022). Unmasking Autism. Harmony Books.
- Raymaker, D. M., et al. (2020). Defining autistic burnout. Autism in Adulthood, 2(2), 132-143.
- Strang, E., & Sakdalan, J. (2025). NDA-DBT pilot study. Autism in Adulthood (SAGE).
- Wilbarger, P., & Wilbarger, J. L. (2002). The Wilbarger approach to treating sensory defensiveness. F. A. Davis.
New articles, directly to your inbox
Neuro-affirming content on ADHD, autism, AuDHD and PDA
— no spam, no aggressive frequency.

Explore interactive resources
More in this series

Next Steps
If this resonated, here are practical ways to go deeper.

