NEURO-AFFIRMING THERAPY · PART 1
"Different" Doesn't Mean "Broken": The Principles of Neuro-Affirming Therapy
The paradigm shift, double empathy, the spiky profile — the principles of neuro-affirming therapy for neurodivergent adults.

"You're too sensitive." "You're overcomplicating things." "Why can't you just be like everyone else?" — messages many neurodivergent adults have heard their entire lives
If you've been hearing these phrases for as long as you can remember, it makes sense that you may have come to believe something is wrong with you. That your reactions are exaggerated. That the way you function is inadequate. That you need to change yourself to fit in.
But what if we looked at this from a completely different perspective? What if your difficulties didn't reflect a personal defect, but a fundamental mismatch between you and an environment that was never built for the way you process the world?
The mismatch is not a personal defect
We live in a world designed for a particular type of neurological functioning — the neurotypical kind. Open-plan offices, rigid schedules, unwritten social rules, the expectation to "perform" consistently at the same level — none of these are universal standards. They are cultural conventions, built around the statistical majority.
When a neurodivergent adult experiences burnout, anxiety, or difficulties with emotional regulation, the cause is rarely "something wrong" with that person. More often, it is the result of a continuous, invisible effort to navigate an environment that was never designed with their neurological needs in mind.
The neurodiversity paradigm (Singer, 1998; Walker, 2014) proposes a fundamental shift: neurodivergence is not a pathology to be corrected, but a natural variation of human functioning — just as legitimate as any other form of diversity.
This perspective does not deny real difficulties. It does not say everything is "fine" and that you don't need support. It says something else entirely: that the source of most difficulties is not in your brain, but in the mismatch between your brain and the demands of the environment.
Robert Chapman proposes an ecological-functional model showing that disability arises from the mismatch between an individual and an environment built for the majority — not from the individual themselves. A recent meta-analysis (Andoni et al., 2024) confirms that effective interventions for autistic adults must completely abandon the deficit model, relying instead on sensory accommodations, strengths recognition, and empowerment of autistic identity.
· · ·
The paradigm shift: from deficit to identity
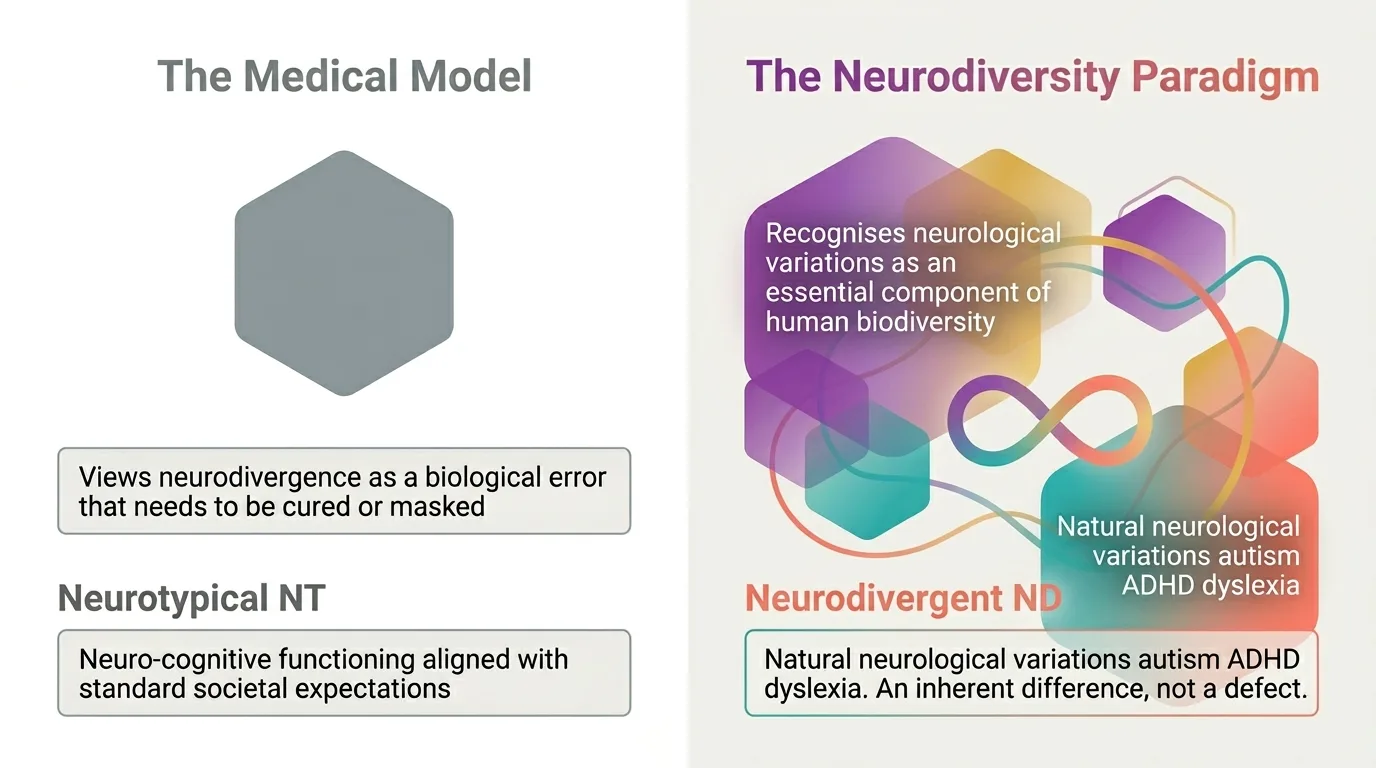
For over a century, neurodivergence was viewed exclusively through the medical lens: a set of "defects" to be diagnosed and "corrected". The medical model reduces the person to a list of symptoms — ignoring context, identity, and lived experience.
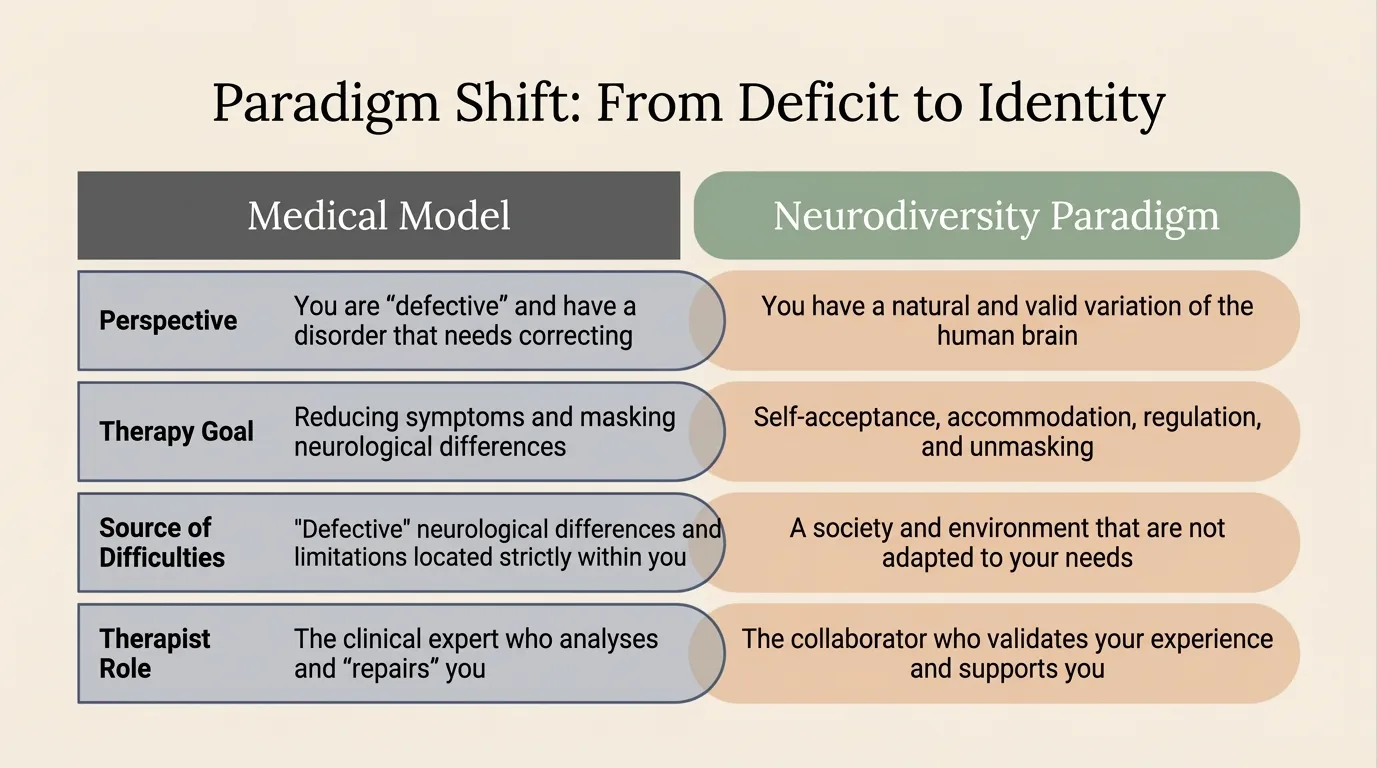
Infographic: The fundamental comparison — Medical Model vs. Neurodiversity Paradigm
Infographic: Medical Model vs Neurodiversity Paradigm The difference is not merely semantic. The way you view neurodivergence determines the way you approach it therapeutically:
THE MEDICAL MODEL "You are defective and have a disorder that needs to be fixed" The goal of therapy: reducing symptoms and masking neurological differences. The therapist is the clinical expert who analyses and "repairs" you.
THE NEURODIVERSITY PARADIGM "You have a natural and valid variation of the human brain" The goal of therapy: self-acceptance, accommodation, regulation, and unmasking. The therapist is a collaborator who validates your experience and supports you.
This shift in perspective does not mean ignoring suffering. It means no longer confusing the source of the suffering: the problem is not your brain — the problem is a society and an environment that are not adapted to your needs.
Explore this interactively: Deficit vs. neuro-affirming language — 5 concrete reframing examples, on the Approach page.
· · ·
The Evolution of Therapeutic Approaches
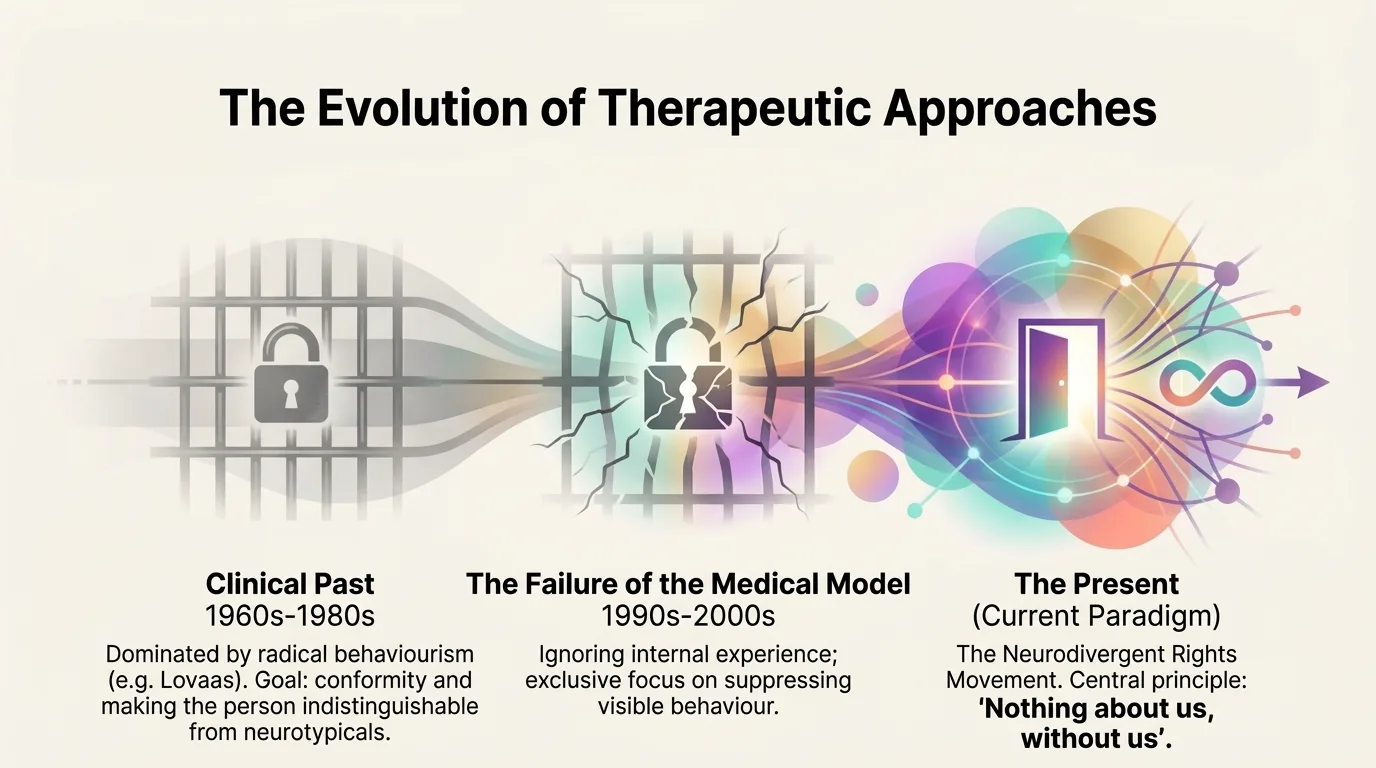
Infographic: Evolution of therapeutic approaches — from behaviorism to the current paradigm 1960s–1980s The Clinical Past Dominated by O. Ivar Lovaas's radical behaviorism, the stated goal was to make the autistic child "indistinguishable from their normal peers." Neurodivergent behavior was seen as an "error" to be corrected, completely ignoring internal emotional and sensory causes.
1990s–2000s The Failure of the Medical Model Exclusive focus on suppressing visible behavior while ignoring internal experience. Compliance-based therapies produced complex trauma and internalized stigma.
THE CURRENT PARADIGM The Neurodiversity Rights Movement The central principle: "Nothing about us, without us." Authentic therapy is built on validation, absolute autonomy, not normalization.
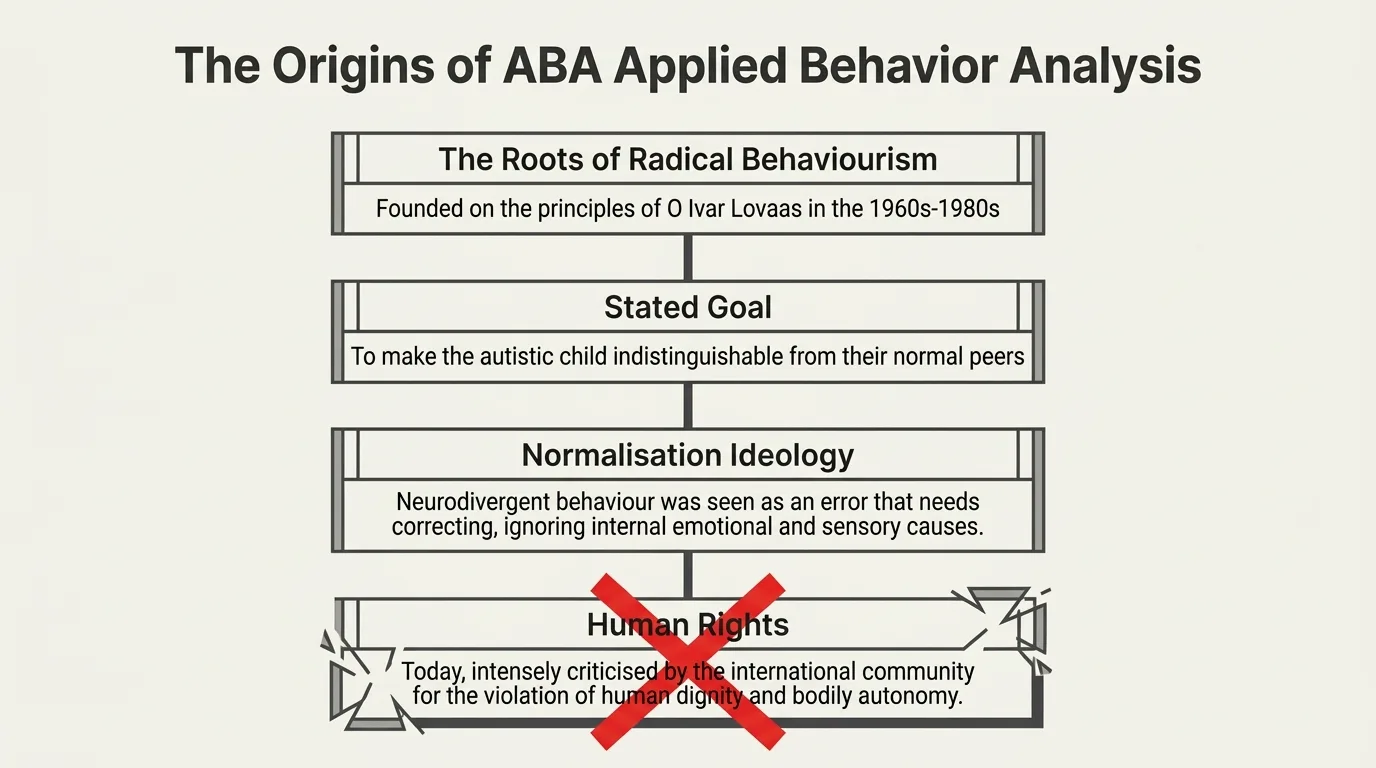
Infographic: The origins of ABA — Applied Behavior Analysis
Ethically Rejected Practices
Compliance training Suppression of stimming Contingent reinforcement Forced eye contact All represent violations of bodily autonomy (Kupferstein, 2018; Pearson & Rose, 2021).
· · ·
What is neuro-affirming therapy, really?
Neuro-affirming therapy is not a specific technique (like CBT or EMDR). It is a lens — a fundamental way in which the therapist sees the world and the person in front of them. It starts from a simple but radical premise: neurodiversity is a natural part of human diversity, not a pathology.
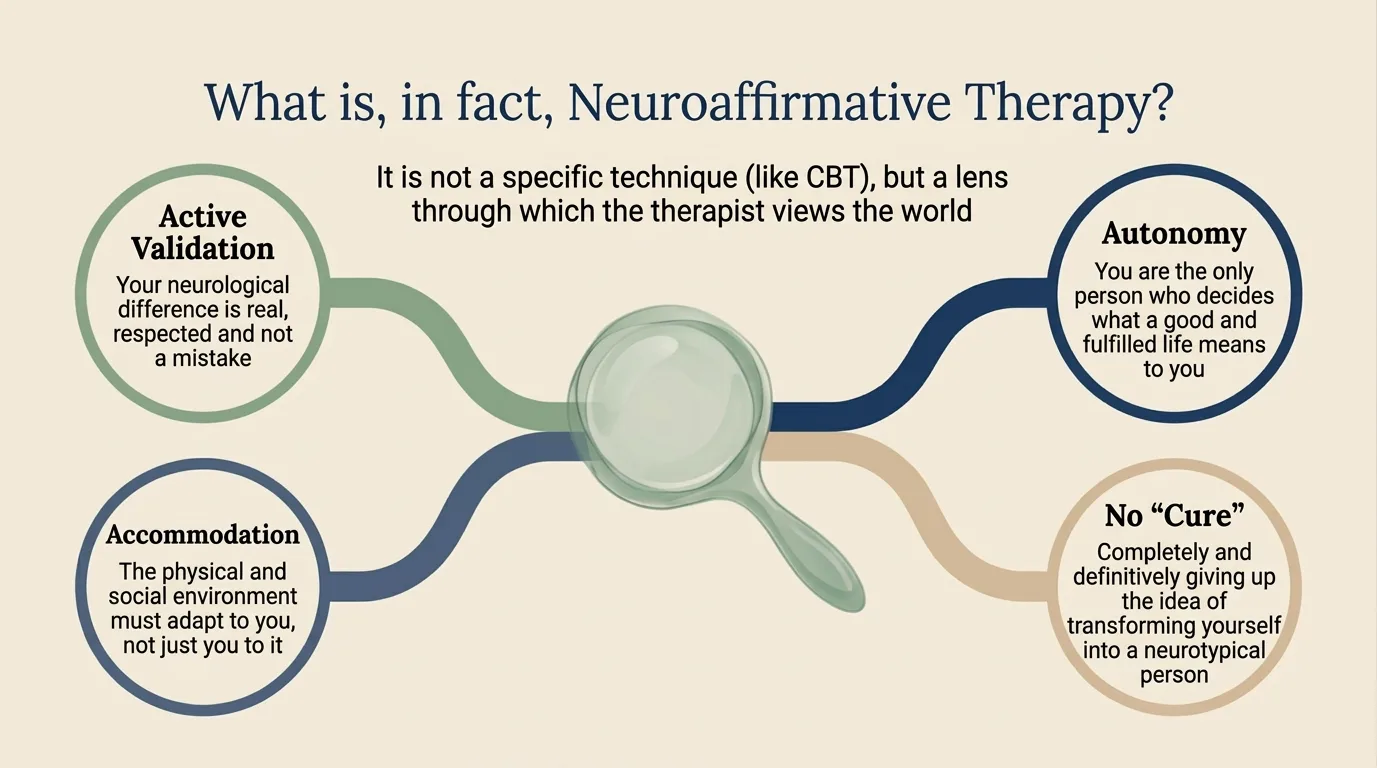
Infographic: The 4 pillars of neuro-affirming therapy
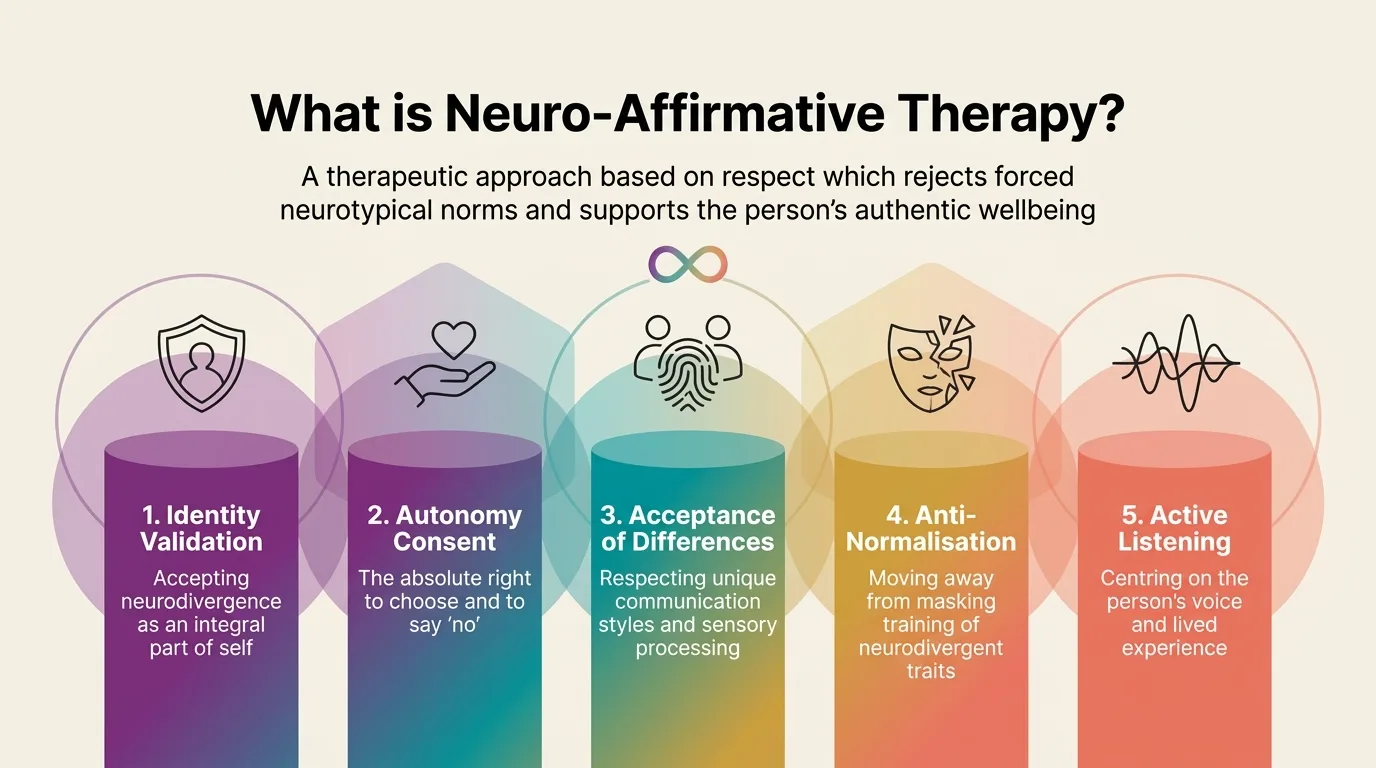
Infographic: The 5 principles of neuro-affirming therapy
PRINCIPLE 1 Active Validation Your neurological difference is real, respected, and not a mistake. We don't explore who you 'should' be — but who you truly are, beyond the masks. Validation isn't just a therapeutic gesture — it's the foundation upon which any authentic progress is built. Without it, therapy becomes yet another stage where you have to perform.
PRINCIPLE 2 Accommodation The physical and social environment must adapt to you, not just you to it. This includes the therapeutic space itself — lighting, sounds, communication style, pacing. If the screen light bothers you, we adjust it. If you need breaks, we take them. If you process better in writing, we work in writing.
PRINCIPLE 3 Autonomy You are the only one who decides what a good and fulfilling life means for you. We don't impose neurotypical standards of 'functionality' or 'success'. Therapeutic goals are yours — not a textbook's, not society's, not the therapist's.
PRINCIPLE 4 No "Cure" The complete and definitive abandonment of the idea of transforming you into a neurotypical person. We don't 'fix' anything — because you're not broken. Your neurodivergence isn't a disease to treat, but a fundamental part of your identity that deserves to be understood and supported.
PRINCIPLE 5 Active Listening Centering the person's voice and lived experience. The therapist doesn't impose external interpretations but listens with genuine curiosity to how the client experiences the world — sensorially, emotionally, and relationally.
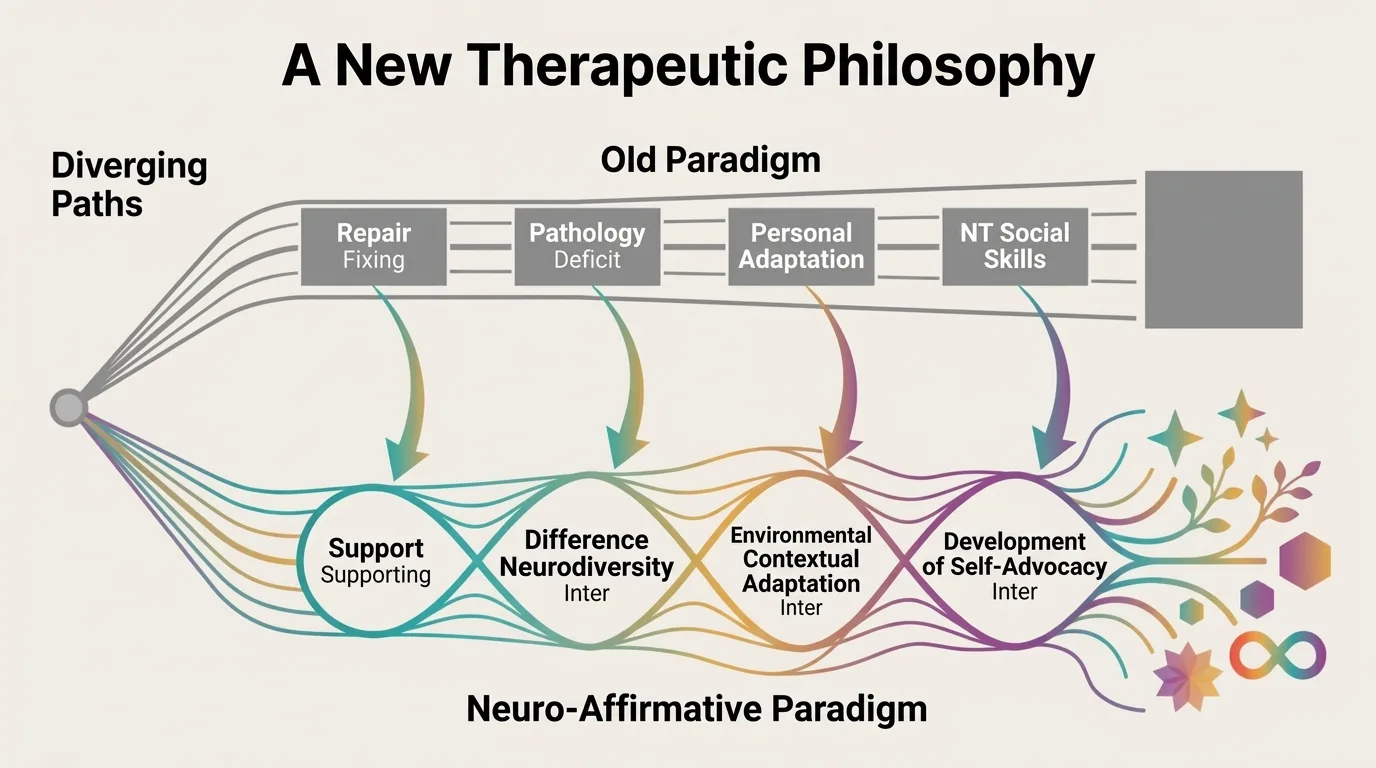
Infographic: A new therapeutic philosophy — from fixing to supporting Julie Roberts proposes a practical neuro-affirmative framework that represents a real alternative to the classic neurotypical "social skills" training. Instead of forcing neurodivergent people to imitate neurotypical communication, the Roberts framework emphasizes authentic social communication — respecting each person's natural style and building bidirectional bridges of understanding.
· · ·
The Double Empathy Problem
For decades, the communication difficulties of autistic people were presented as a unidirectional deficit — a problem that lies solely within the autistic person. Theories such as "Theory of Mind" claimed that autistic people cannot understand others' intentions or emotions.
Recent research has completely overturned this model.
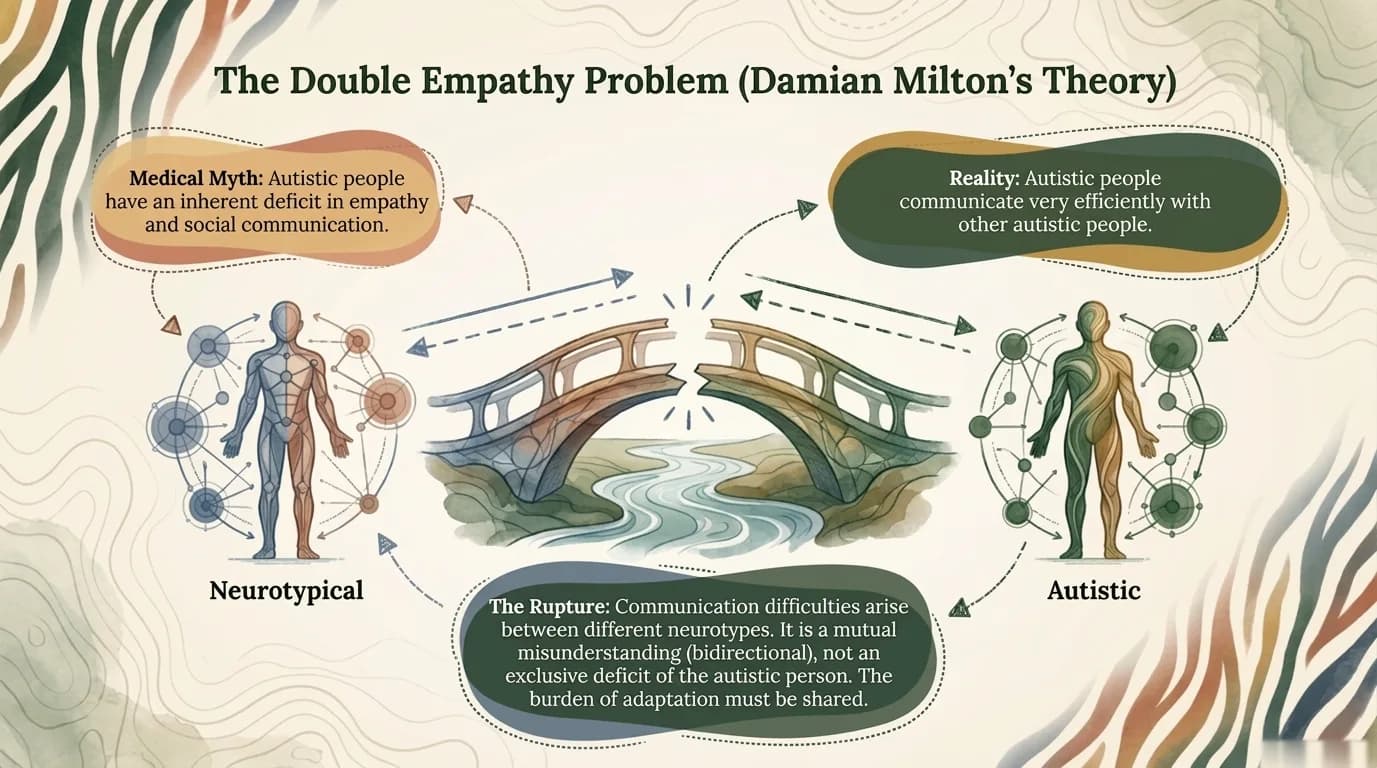
Infographic: Double Empathy — communication difficulties arise between different neurotypes, not from a one-sided deficit In 2020, Crompton and colleagues experimentally demonstrated something autistic people had known intuitively all along: communication between autistic people works just as well as communication between neurotypical people. Problems arise at the interface — when two neurologically different communication styles interact without understanding each other.
THE MEDICAL MYTH "Autistic people have an empathy deficit" The difficulty belongs to the autistic person. They need to be taught to communicate "correctly" — meaning neurotypically.
THE REALITY (Milton, 2012) "The difficulty is bidirectional" Communication between different neurotypes is like running an iOS app on an Android system. It's not your fault — it's a compatibility issue.
This is not just an academic nuance. It has profound implications for therapy. If communication difficulties are not a deficit within the autistic person, then the solution is not to "train" the person to communicate neurotypically — but to build bridges of understanding in both directions.
This is exactly the principle at the heart of my therapeutic approach: I don't ask clients to adapt to me. I adapt to them.
Recent evidence strengthening the theory
A study of 81 adults (Cheang et al., 2024) demonstrated that non-autistic people score significantly lower on empathic accuracy when viewing autistic narrators — especially for emotions like joy or sadness. In other words, "mind-blindness" goes both ways.
Morrison et al. (2019) showed that neurotypical people rate their first interaction with autistic partners far less favorably than interactions with other neurotypicals. Jones et al. (2023) confirmed that mixed conversations (autistic-neurotypical) are perceived as "awkward" by external observers, while same-neurotype interactions are rated as smooth and pleasant.
Heasman and Gillespie (2019) demonstrated that in autistic-autistic conversations, autistic people easily build shared understanding and excellent rapport — confirming that the difficulties aren't the individual's, but arise at the intersection of different neurotypes.
The Triple Empathy Problem
Shaw et al. (2023) extended Milton's concept by introducing the "Triple Empathy Problem" in healthcare. Beyond the neurological barrier (autistic vs. neurotypical), there's a third gap: medical culture, specialist jargon, and the administrative rigidity of healthcare systems.
This concept explains why many autistic adults avoid healthcare entirely (Doherty et al., 2022) — the hostile sensory environment in clinics, unclear communication, and lack of accommodation transform each visit into an overwhelming experience.
— Damian Milton (2012)"When people with very different experiences of the world interact with one another, they will struggle to empathize with each other."
· · ·
What it does differently from standard therapy
Many neurodivergent adults leave therapy feeling judged or treated as projects to be "fixed". When a therapist doesn't understand that the way you process the world is different — not defective — the entire therapeutic process can become yet another source of invalidation.
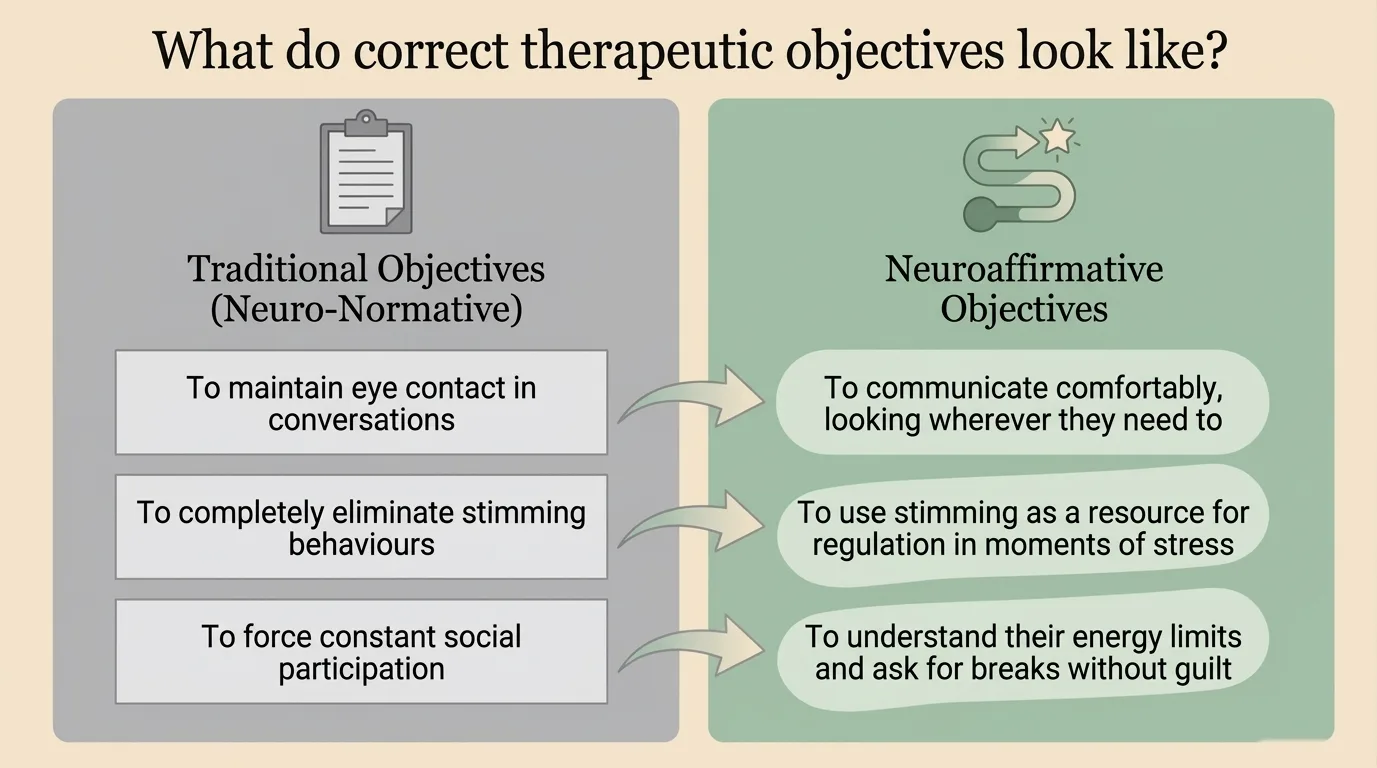
Infographic: Therapeutic goals — from conformity to self-regulation
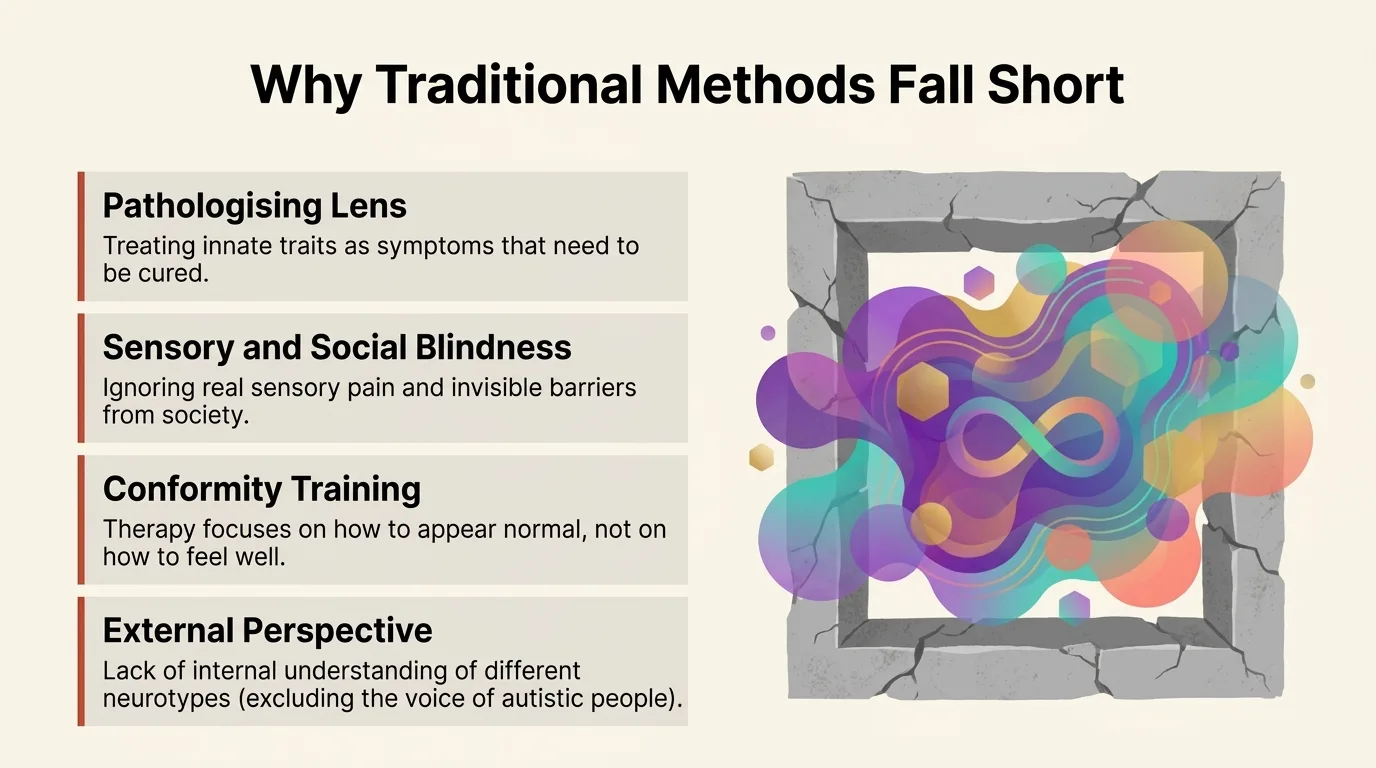
Infographic: Why traditional methods fail Here is what a neuro-affirming approach does differently, in concrete terms:
Standard therapy Neuro-affirming therapy "You need to learn to make eye contact" "Eye contact is optional. We communicate in whatever way works for you" "Your social anxiety needs to be treated" "Let's explore whether this is anxiety or sensory overload" "You need to manage your emotions better" "Your emotions make sense. Let's understand them, not suppress them" "You need to be more organised" (ADHD) "Let's build systems that work with your brain, not against it" "Stimming is a behaviour to be eliminated" "Stimming is self-regulation. You can do it during sessions too" Behavioural activation as a response to withdrawal Assessing whether withdrawal is necessary protection, not "avoidance" Focus on "social skills" to be acquired Focus on mutual understanding (Double Empathy) Objective: normalization Objective: well-being and autonomy Assessment: external perspective (how NT sees it) Assessment: internal perspective (how the ND person feels) Manages "problem behavior" Supports hidden needs and regulation The essential difference: in standard therapy, the client is the one who needs to adapt — to the therapist, to the method, to social norms. In neuro-affirming therapy, the therapy adapts to the client.
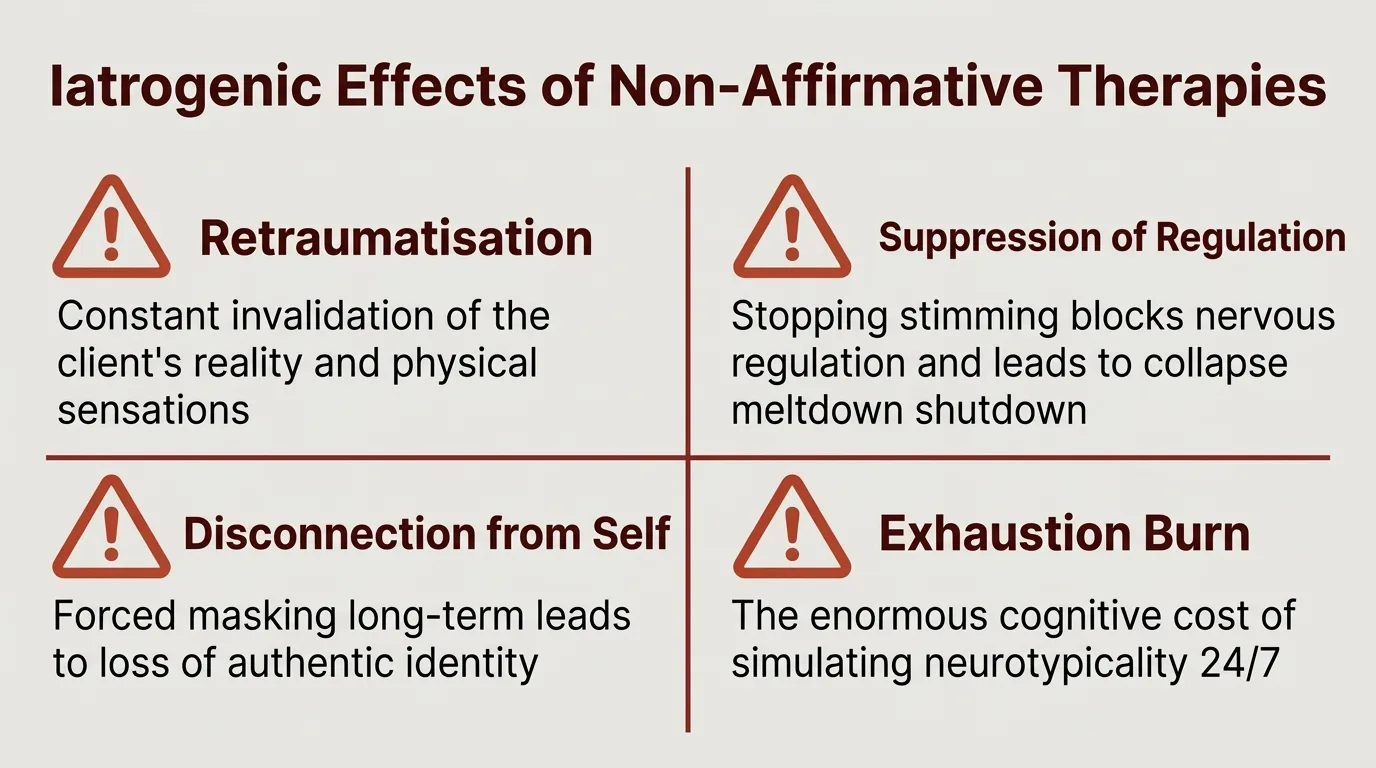
Infographic: Iatrogenic effects of non-affirmative therapies
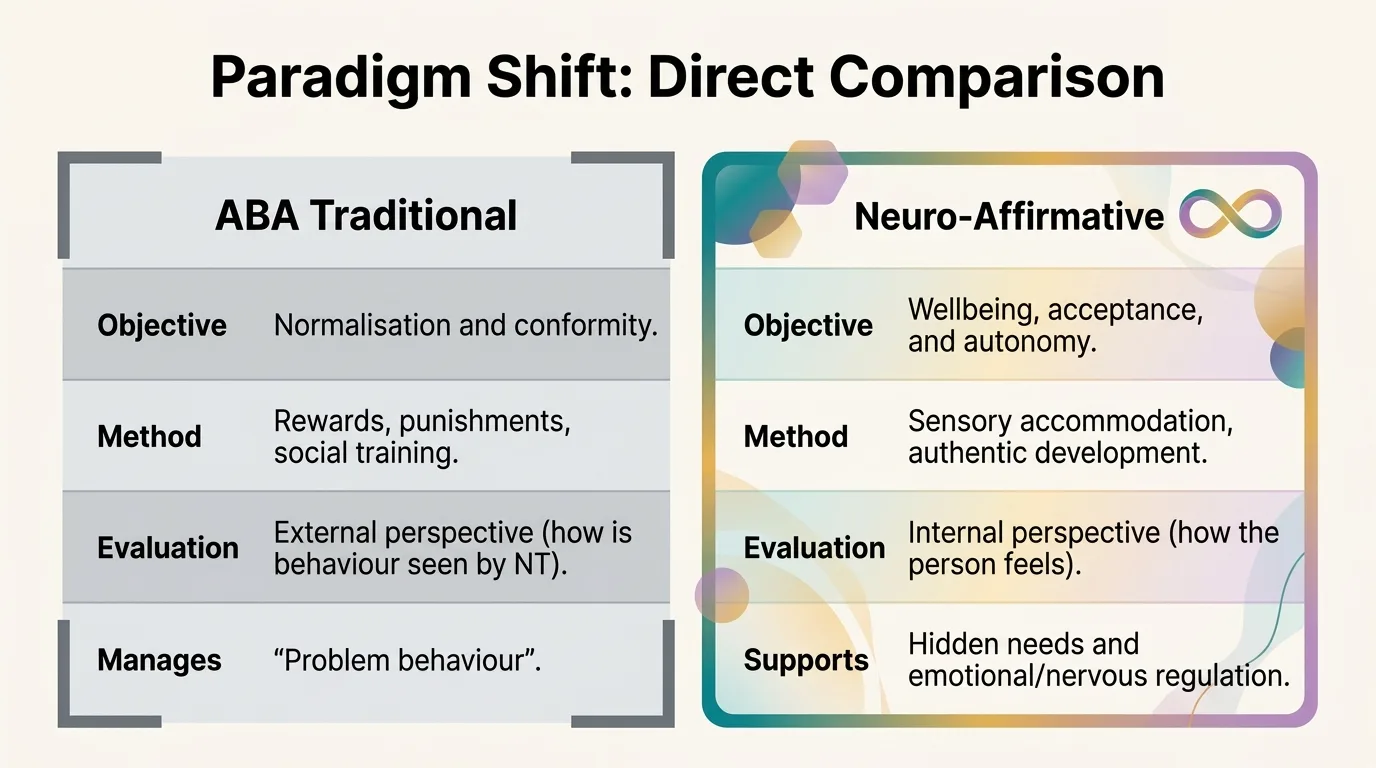
Infographic: Direct comparison — ABA vs Neuro-Affirming · · ·
These differences become even more apparent when we look at how each approach understands individual variability.
The Spiky Profile: why "one size fits all" doesn't work
One of the most important concepts I explain to my clients is the spiky profile. Neurodivergent people don't function on a straight line between "mild" and "severe". They have a dramatically uneven profile — with peaks of excellence and valleys of difficulty, sometimes in surprisingly adjacent areas.
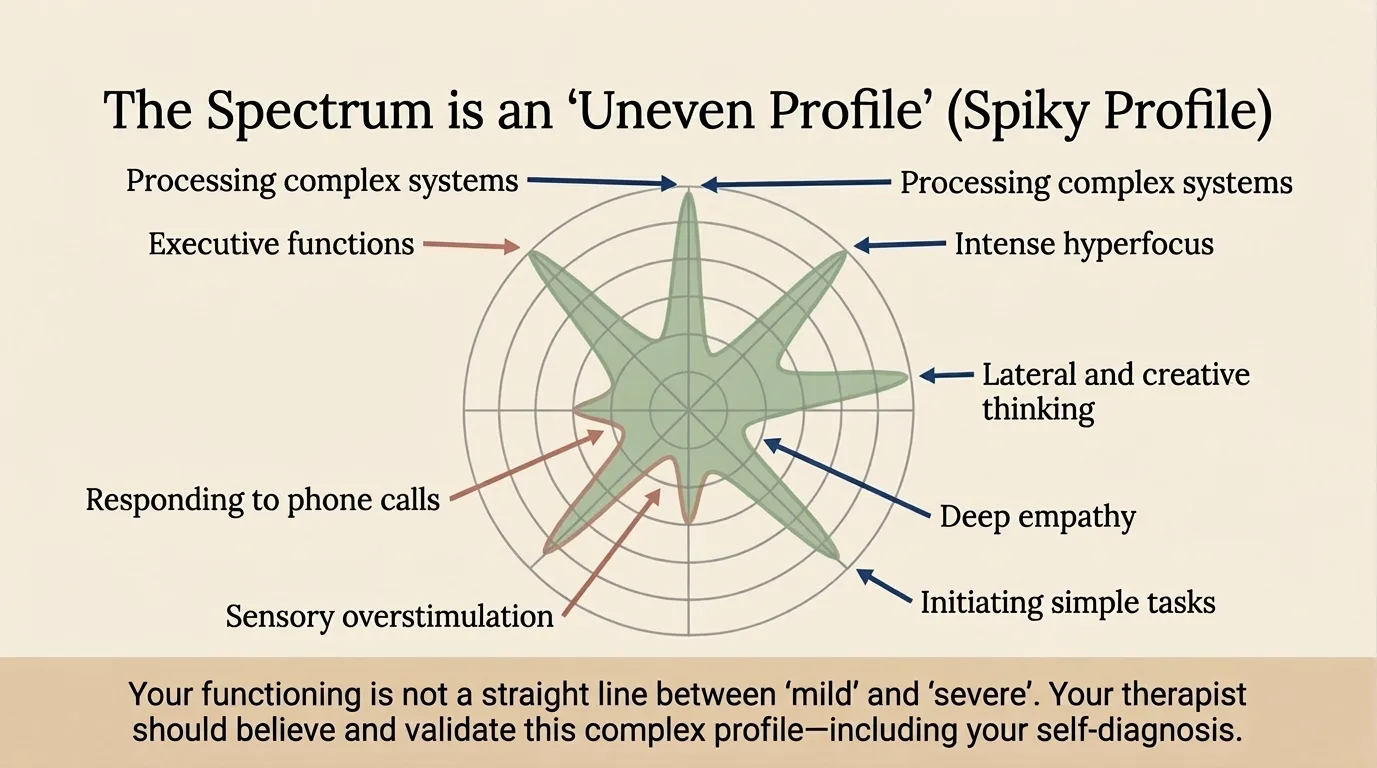
Infographic: The Spiky Profile — your functioning is not a straight line between "mild" and "severe" You can be brilliant at processing complex systems and completely overwhelmed by initiating simple tasks. You can have deep empathy and intense hyperfocus, yet be unable to answer a phone call. You can have creative lateral thinking, but executive function — that "basic" ability to start, organise, and complete — may be a constant challenge.
This is why the "one size fits all" approach in standard therapy fails so often with neurodivergent clients. A therapist who doesn't understand the spiky profile sees contradictions where, in fact, there are characteristics of the same nervous system.
Monotropism theory (Murray, Lesser & Lawson, 2005) provides the scientific foundation: autistic attention is intensely channeled toward stimuli of internal interest, enabling an extraordinary capacity for hyperfocus — not a deficit, but a source of excellence.
Russell et al. (2019) documented how autistic adults identify their own strengths: hyperfocus, attention to detail, excellent memory, loyalty, and deep empathy. Han et al. (2023) emphasize heterogeneity: "If there are 6 million autistic people, you have 6 million different types" — confirming that no universal approach can work.
"I'm a normal zebra, not a weird horse" — Brianna Morton, explaining why neurotypical standards cannot be universally applied.
Your therapist needs to believe and validate this complex profile — including your self-diagnosis. If you can process complex systems but can't initiate simple tasks, you are not "lazy". You are neurodivergent, and your strategies need to be built for your profile, not for a statistical average.
Explore this interactively: Neurodivergence as a multidimensional spectrum — 6-axis radar chart with 3 neurodivergent profiles (Autism, ADHD, AuDHD). On the Approach page.
This was Part 1 — the foundations of neuro-affirming therapy. In Part 2, we explore how it works in practice: the cost of masking, the sensory safety pyramid, what a session looks like, the integrative approach, and the signs that help you recognise the right therapist.
References
- Andoni, A. et al. (2024). Interventions for autistic adults: A meta-analysis. Autism Research.
- Chapman, R. (2021). Neurodiversity Theory and Its Discontents: Autism, Schizophrenia, and the Social Model of Disability. In Bertilsdotter Rosqvist, H., Chown, N., Stenning, A. (Eds.), Neurodiversity Studies. Routledge.
- Cheang, R. et al. (2024). Empathic accuracy and autism: Non-autistic adults are less accurate at reading autistic emotions. Cognition and Emotion.
- Crompton, C.J., Ropar, D., Evans-Williams, C.V., Flynn, E.G., & Fletcher-Watson, S. (2020). Autistic peer-to-peer information transfer is highly effective. Autism, 24(7), 1704-1712.
- Doherty, M. et al. (2022). Barriers to healthcare for autistic adults: Consequences & policy implications. British Journal of General Practice, 72(721), e46-e48.
- Han, E. et al. (2023). Autistic heterogeneity: Linking theories of autism with assessment and intervention practice. Journal of Autism and Developmental Disorders.
- Heasman, B. & Gillespie, A. (2019). Neurodivergent intersubjectivity: Distinctive features of how autistic people create shared understanding. Autism, 23(4), 910-921.
- Jones, D.R. et al. (2023). Observers' perceptions of interactions between autistic and non-autistic adults. Autism.
- Kupferstein, H. (2018). Evidence of increased PTSD symptoms in autistics exposed to applied behavior analysis. Advances in Autism, 4(1), 19-29.
- Milton, D.E.M. (2012). On the ontological status of autism: the 'double empathy problem'. Disability & Society, 27(6), 883-887.
- Morrison, K.E., DeBrabander, K.M., Jones, D.R., Faso, D.J., Ackerman, R.A., & Sasson, N.J. (2019). Outcomes of real-world social interaction for autistic adults paired with autistic compared to typically developing partners. Autism, 24(5), 1067-1080.
- Morton, B. (2020). The Zebra Analogy: Rethinking Neurodivergent Identity. [Social media / advocacy communication].
- Murray, D., Lesser, M. & Lawson, W. (2005). Attention, monotropism and the diagnostic criteria for autism. Autism, 9(2), 139-156.
- Pearson, A. & Rose, K. (2021). A conceptual analysis of autistic masking: Understanding the narrative of stigma and the illusion of choice. Autism in Adulthood, 3(1), 52-60.
- Pellicano, E. & den Houting, J. (2022). Annual Research Review: Shifting from 'normal science' to neurodiversity in autism science. Journal of Child Psychology and Psychiatry, 63(4), 381-396.
- Russell, G. et al. (2019). Mapping the autistic advantage from the accounts of adults diagnosed with autism. Disability & Society, 34(7-8), 1089-1111.
- Shaw, S.C.K. et al. (2023). The triple empathy problem: Autistic people and healthcare. British Journal of General Practice.
- Singer, J. (1998). Odd People In: The Birth of Community Amongst People on the Autistic Spectrum. Thesis, University of Technology, Sydney.
- Walker, N. (2014). Neurodiversity: Some basic terms & definitions. Neurocosmopolitanism.
New articles, directly to your inbox
Neuro-affirming content on ADHD, autism, AuDHD and PDA
— no spam, no aggressive frequency.

Explore interactive resources
More in this series

Next Steps
If this resonated, here are practical ways to go deeper.