BURNOUT · PART 2
The Anatomy of Neurodivergent Burnout — Part 2
Masking, interoception and the invisible mechanisms that lead to neurodivergent burnout. Part 2 of the neuroaffirmative series.
———
Having established in the first part that neurodivergent burnout is a condition distinct from depression, in this part we will explore the internal mechanisms that make the breakdown seem ‘sudden’ and ‘inexplicable’. We will focus on the ‘invisible triad’ that sabotages the ability to self-monitor: Interoception, Alexithymia and Masking.
Why didn’t I see it coming?
The aim of this module is to answer the painful question: “Why didn’t I see it coming?”. Many neurodivergent people blame themselves for the breakdown, believing they were not resilient or capable enough. Here we will demonstrate that the problem is not one of willpower or character, but a matter of biological ‘hardware’ and ‘software’. We will explore why the body’s standard warning systems typically do not function in neurodiversity and how this allows massive stress to build up, completely unnoticed, until the critical moment of functional breakdown.
Why does the breakdown appear ‘sudden’?
The breakdown is not sudden – it only appears so from the outside (and sometimes from the inside). The battery analogy helps: a flat battery does not simply stop when we want it to; it discharges gradually but continuously. The difference is that in neurodiversity, the ‘battery level indicator’ is faulty. The three causes of this ‘faulty indicator’ are: Different interoception, Alexithymia and Masking. Together, they create a ‘false screen’ that shows ‘everything is fine’ when, in fact, the body is running on reserves of cortisol and adrenaline.
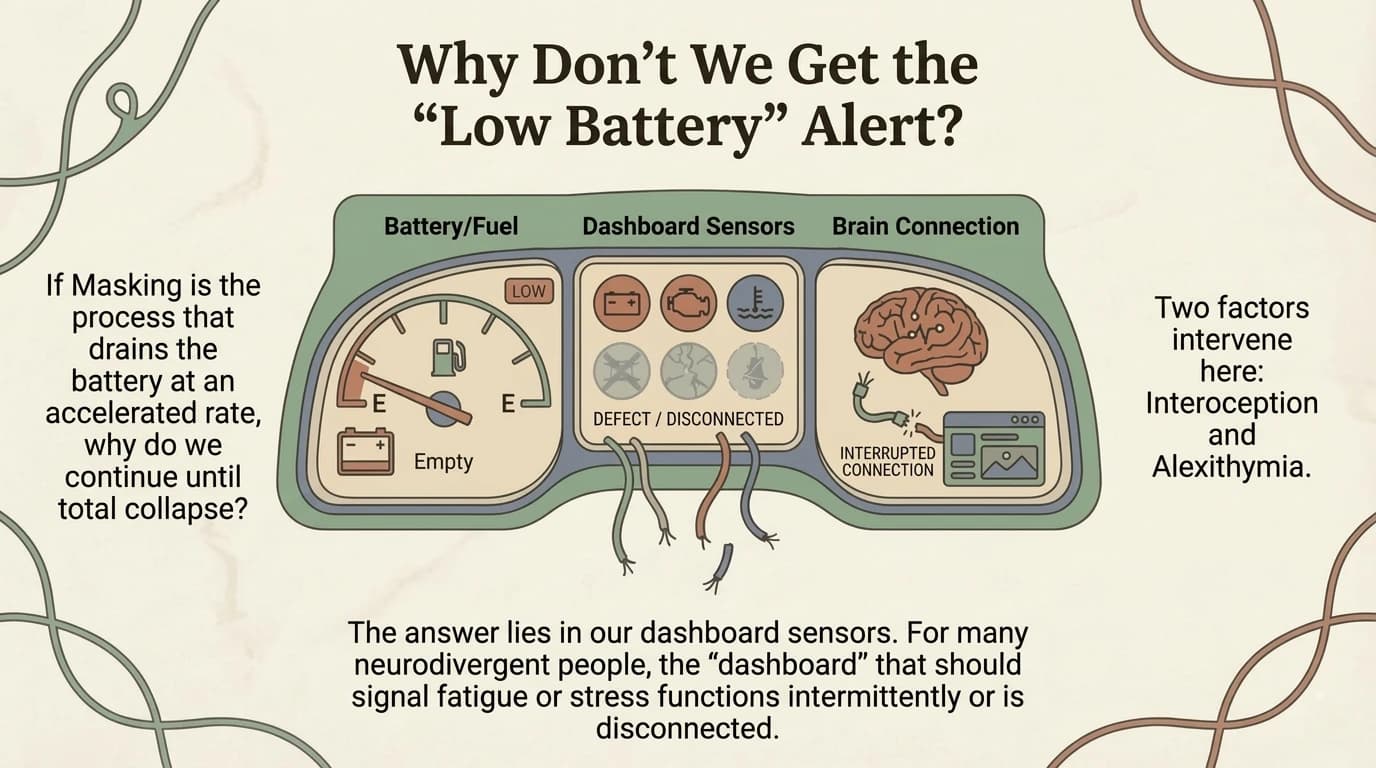
Why don’t we get the ‘Low Battery’ alert?
This is the central question: if burnout comes with so many biological signals, why don’t we see them? The answer lies in the paradox of a turbo engine with disconnected sensors. The neurodivergent brain often operates at higher revs (more intense processing, hypervigilance, over-analysis), but at the same time, the feedback system that should report the ‘fuel level’ functions differently – and often with a critical delay or distorted signals.
The Unseen Cause #1: Interoception — The 8th Sense
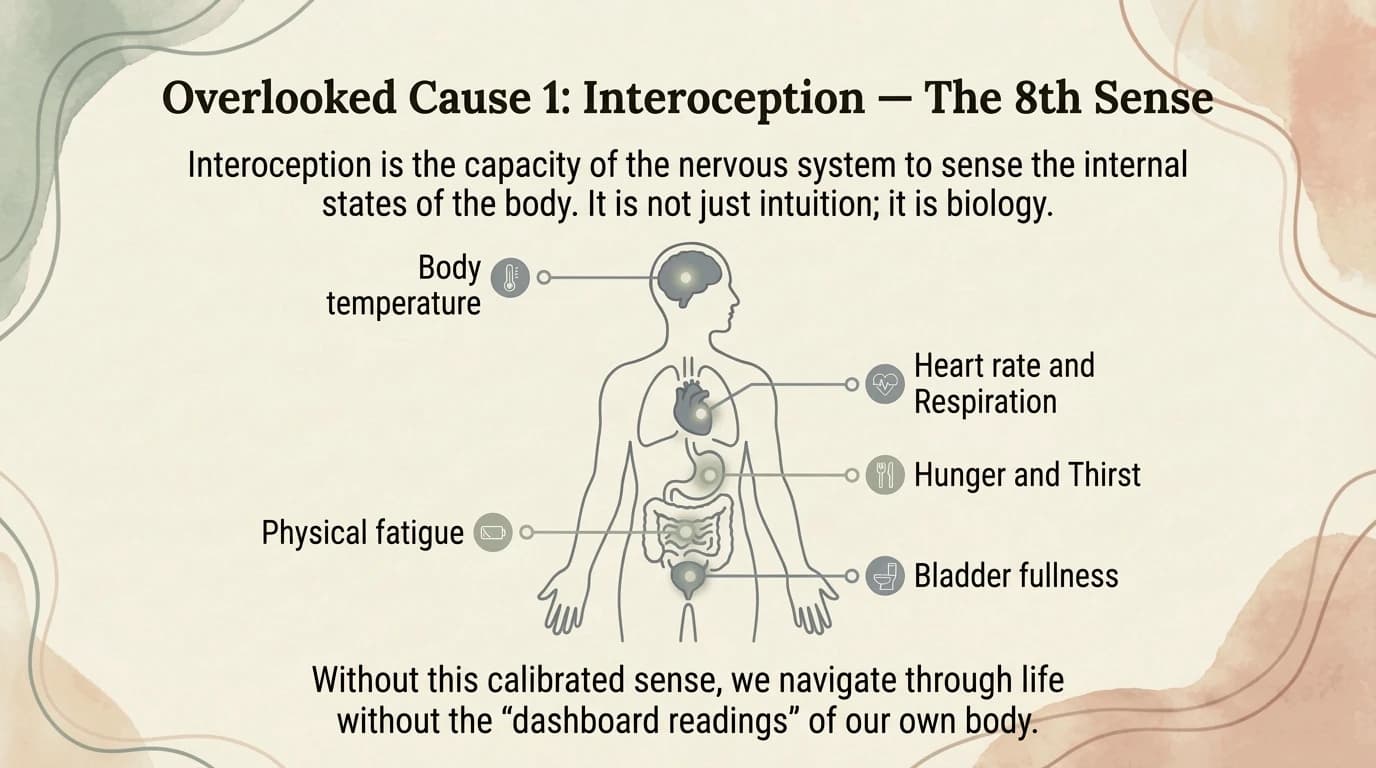
Interoception is the ‘internal sense’ — the brain’s ability to receive, interpret and integrate signals from the body (hunger, thirst, temperature, fatigue, pain, muscle tension, the need to go to the toilet, etc.). Anatomically, the insula (a deep region of the cerebral cortex) is the interoceptive ‘thermostat’. Research shows significant differences in insular activation in people with autism (DuBois et al., 2016). If the thermostat is calibrated differently, you won’t know you’re about to overheat the engine. This is the ‘physiological blindness’ that allows stress to build up silently.
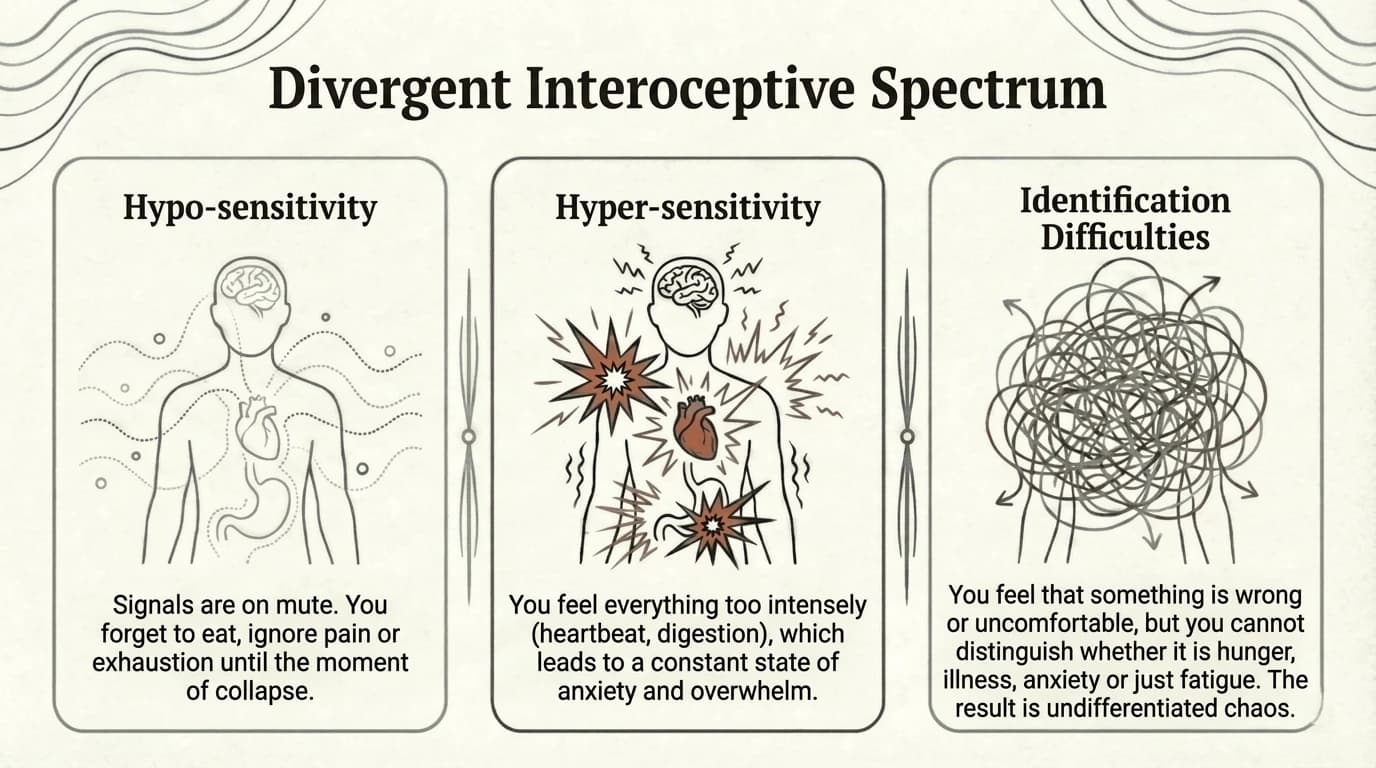
The Divergent Interoceptive Spectrum
Interoception is not “all or nothing”. There are three main profiles:
- Hyposensitivity: “I don’t feel anything until it’s too late” — I don’t recognise hunger, tiredness or physical pain until it reaches a critical level.
- Hypersensitivity: “I feel everything, all the time, at full intensity” — Every internal sensation is amplified, creating a state of perpetual alertness.
- Difficulty identifying: “I feel something, but I don’t know what” — Sensations are present, but the brain cannot classify them correctly (hunger vs. anxiety vs. tiredness).
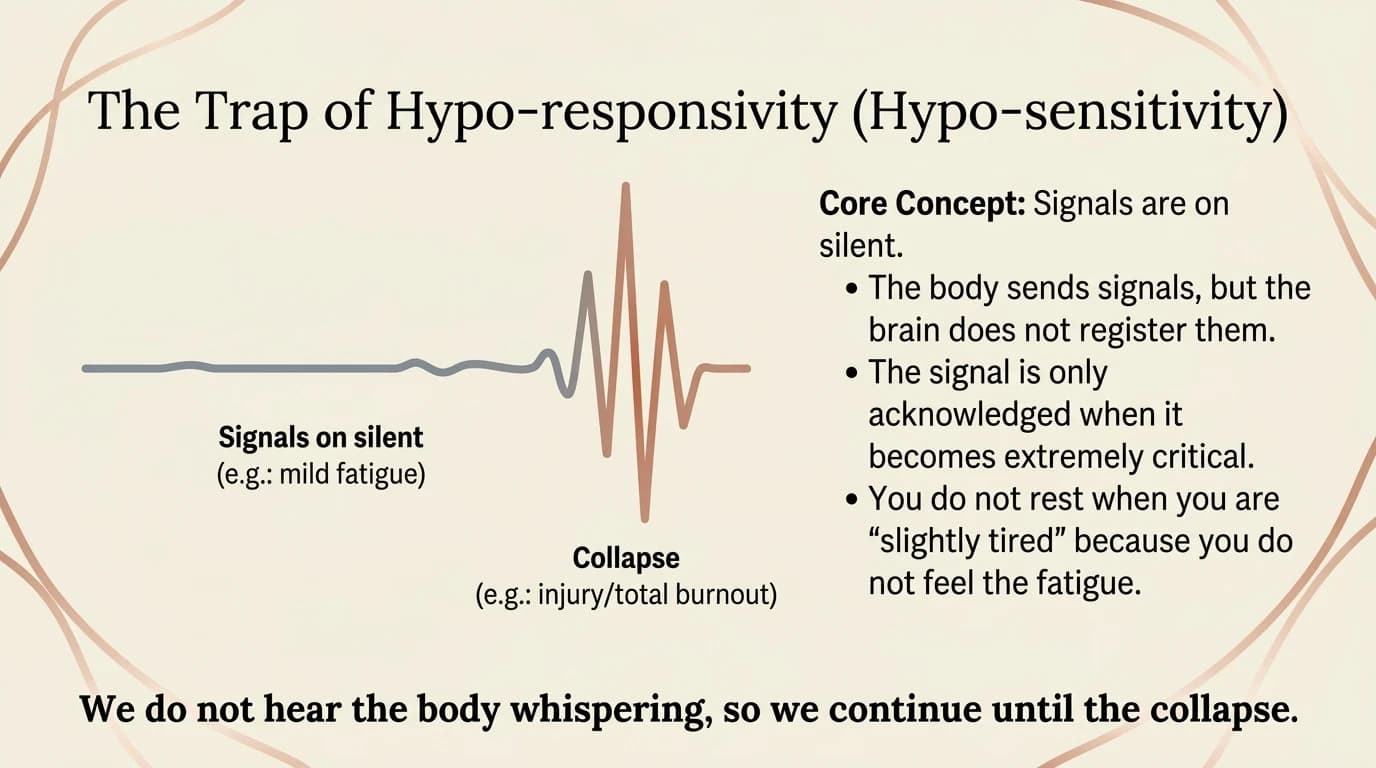
The Hypersensitivity Trap
This profile is the most dangerous for burnout because it operates on an ‘all or nothing’ principle: We don’t hear the body ‘whispering’ (subtle signals of tiredness, tension, hunger). We continue to function seemingly normally (even excellently!) because we have no negative feedback. When the body finally “screams” (meltdown, shutdown, physical collapse), it is already too late for preventive intervention. In practice, we are living on “energy credit” without realising it: we are spending energy we don’t have, because we don’t know we don’t have it.
Interoceptive Hypersensitivity
At the opposite end of the spectrum, interoceptive hypersensitivity creates its own type of exhaustion. Here, the volume is stuck on maximum: every sensation is amplified and urgent. The brain receives a constant stream of alarms, but cannot distinguish between a genuine emergency and minor discomfort. The result: a chronic state of fight-or-flight based on internal, not external, signals. The person is literally at war with their own body. Exhaustion comes not from a lack of signals, but from their uncontrollable excess. The nervous system cannot ‘switch off’ – it is in a perpetual state of crisis, leading to a different but equally devastating burnout.
Undifferentiated Chaos: Difficulties in Identification
This third profile is the most confusing: sensations are present, but the brain cannot classify them. The person feels ‘something’ in their body, but cannot determine whether it is hunger, anxiety, sadness, tiredness or illness. Every internal signal requires ‘manual translation’ — a considerable cognitive effort to decipher what one’s own body is signalling. This extra effort consumes cognitive bandwidth, leaving fewer resources for the day’s tasks. Over time, many people give up on ‘translation’ and ignore the signals entirely — a coping mechanism that results in the same blindness as hyposensitivity.
The interoceptive paradox in autism
Recent studies reveal a fascinating paradox: people with autism tend to have low objective interoceptive accuracy (difficulty in correctly counting their heartbeats in laboratory conditions), but exaggerated subjective interoceptive sensitivity (they report chronic awareness and overwhelm caused by bodily sensations).
This discrepancy creates a state of constant physiological uncertainty: the body feels an intense level of stimulation, but the brain cannot correctly decode the source. A rapid pulse caused by hunger may be misinterpreted as a panic attack. The constant cognitive effort required to decode these erroneous signals rapidly drains energy and accelerates the onset of burnout.
The Unseen Cause #2: Alexithymia
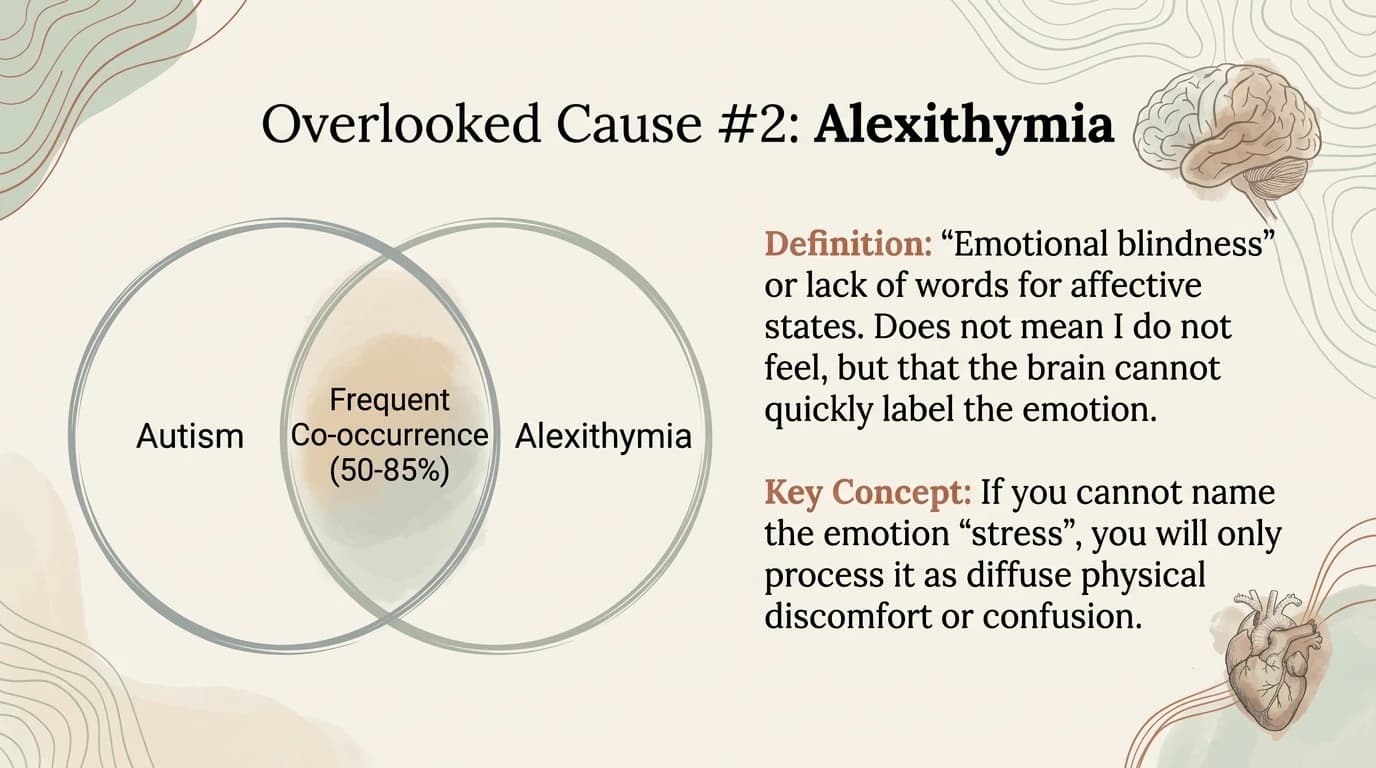
Alexithymia = difficulty in identifying, processing and expressing emotions. Extremely high prevalence (50–85% of people with autism have clinical levels of alexithymia, according to studies by Bird and Cook, 2013; Kinnaird et al., 2019). It is not the absence of emotions, but the inability to ‘read’ and ‘name’ them. The ‘colour box without labels’ analogy: all the colours are present (emotions exist), but the labels (names, classifications) are missing or mixed up. A critical consequence: without emotional awareness, stress becomes ‘somatised’ — manifesting as physical symptoms (headaches, digestive problems, tension) that are often ignored or misdiagnosed.
The Mechanism of Exhaustion through Alexithymia
Stress occurs (event) → The amygdala triggers the stress response (cortisol, adrenaline) → The prefrontal cortex should process and regulate → But alexithymia blocks the identification of the state → Stress remains unprocessed but biochemically active → It accumulates in the body as an ‘allostatic load’. Essentially, the body is in a state of stress, but the mind is unaware of this. Coping mechanisms do not activate because there is no conscious ‘alarm signal’. It is like a fire burning in the basement – the smoke does not reach the smoke detectors upstairs, but the house continues to burn.
The Critical Link: Body and Emotion
Poor interoception = I don’t feel what’s happening in my body. Alexithymia = I don’t know what I’m feeling emotionally. Together, they create a total ‘deadlock’: neither the body nor the emotions send signals clear enough to attract conscious attention. The consequence for burnout: the person has neither somatic nor emotional feedback to warn them that their resources are running out. It is like driving a car without a fuel gauge or a dashboard – you have no way of knowing that you are about to run out of fuel. This makes proactive self-care almost impossible without external monitoring tools.
Key Cause #3: Masking (Social Camouflage)
Masking (or camouflaging) is the third pillar of the invisible triad and is perhaps the best-documented predictor of burnout and suicidal ideation among autistic people (Cassidy et al., 2018; Beck et al., 2020). Masking is not merely ‘being polite’ or ‘fitting in socially’ – it is a complex, often unconscious process of monitoring, suppression and performance that runs constantly in the background, consuming massive cognitive resources. The virtual machine (VM) analogy: like a computer running a second (neurotypical) operating system alongside the native (neurodivergent) one – both consume RAM and CPU, but one is entirely artificial and must be kept active.
Masking – The Cost of Social Safety
Masking is not an act of vanity, but a survival mechanism often developed in childhood to avoid bullying, rejection or punishment. Concrete examples include: suppressing stimming, forcing eye contact, scripting conversations, mimicking facial expressions, tolerating sensory overload without reacting. The cost of this ‘social safety’ is immense: every social interaction becomes a ‘performance’ that requires energy. Over time, masking functions like a pressure cooker – the pressure builds invisibly until it reaches the point of explosion (meltdown) or implosion (shutdown/burnout).
The Invisible Energy Cost of Social Camouflage
Social camouflage is a complex phenomenon, defined by researchers (Hull et al., 2017) through three distinct strategies:
- Compensation: The active development of strategies to ‘compensate’ for social difficulties (preparing conversations, studying social rules, practising facial expressions).
- Masking itself: The active concealment of autistic traits (suppressing stimming, forcing eye contact, controlling tone of voice).
- Assimilation: Attempting to ‘disappear’ into the social environment by imitating others and avoiding any behaviour that might be noticed as ‘different’. Each of these strategies requires constant cognitive energy, resulting in a chronic energy deficit which, over time, precipitates burnout.

Disconnection from the Self
A tragic side effect of long-term masking is the loss of identity and connection with one’s own needs. Many neurodivergent people end up no longer knowing who they truly are, because they have spent so much time performing a neurotypical version of the self. This can lead to a ‘Fawn’ trauma response (Walker, 2013) – an excessive focus on the needs of others, with the systematic neglect of one’s own needs. Rediscovering one’s authentic self is one of the most important – and most challenging – aspects of recovering from burnout. It requires safe spaces, time and often therapeutic support to ‘unmask’ the layers of social camouflage. Recent research confirms a further devastating mechanism: masking not only consumes energy — it actively suppresses interoception. To mask effectively, the autistic person must completely ignore internal signals of discomfort. Long-term practice of camouflage creates a ‘psychological barrier’ between the individual and their own needs, turning the ignoring of pain and fatigue into an automatic response. This forced disconnection makes recovery much more difficult, as the person no longer knows what their needs are.
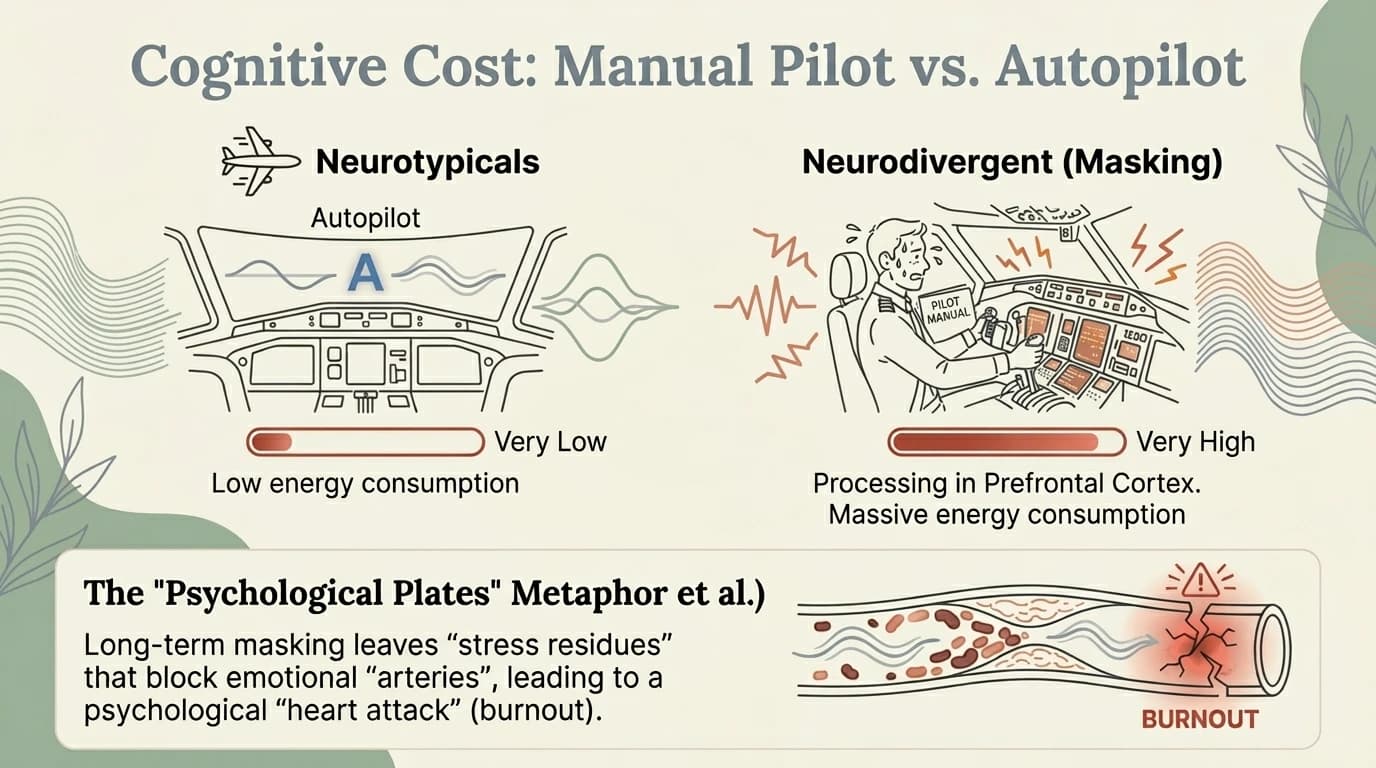
Cognitive Cost: Manual Pilot vs. Autopilot
Autopilot (neurotypical): many social interactions are automated, processed at a subcortical level, requiring minimal effort. Manual Pilot (neurodivergent): the same interactions require conscious, cortical, ‘step-by-step’ processing – vastly more energy-intensive. This concept is linked to the idea of the ‘Mental Board’ (Raymaker et al., 2020): as if every interaction were a workout at the gym – for neurotypicals it’s a stroll, but for neurodivergent people it’s a sprint with obstacles. The fuller the mental plate, the closer one gets to a “mental heart attack” (burnout). Note: Autistic women, people with AuDHD (autism + ADHD) and those diagnosed late are disproportionately affected by burnout — due to amplified social pressure, chronic underdiagnosis and hormonal fluctuations. We will explore these differences in detail in Part 3: External Factors.
The Triad of Invisible Exhaustion: The Perfect Storm
This diagram integrates the three mechanisms into a coherent model: Masking increases the load (it consumes active energy). Deficient interoception cuts the wires of the level sensors (you don’t feel how much you’re consuming). Alexithymia blocks the emotional alarm sensor (you don’t know you’re in danger). When all three operate simultaneously (and for most neurodivergent people, they do), a breakdown becomes a statistical certainty, not a personal failure. It is literally a system designed to collapse – and this is not your fault.
The Disaster Equation: ‘The Perfect Storm’
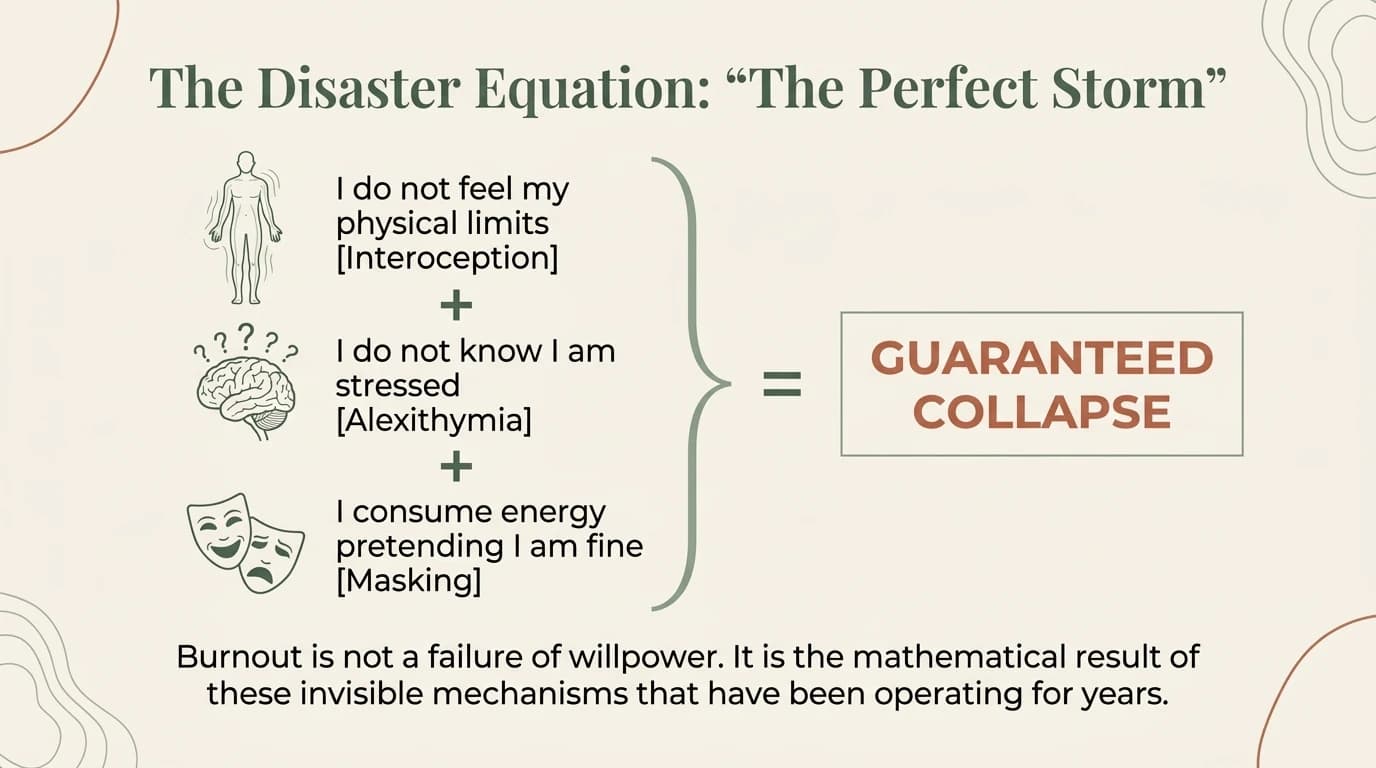
I don’t feel my physical limits (Interoception) + I don’t know I’m stressed (Alexithymia) + I expend energy pretending I’m fine (Masking) = GUARANTEED COLLAPSE. It is vital to understand that this is an equation of resources, not of morality. Burnout is not a failure of willpower. You are not weak because you have ended up here. You are the mathematical result of biological mechanisms and social pressures that have been working against you for years. Healing begins by changing the variables in this equation (reducing masking, improving awareness), not by trying to be ‘stronger’.
You’re not lazy, you’re disconnected
This is an essential reframing for combating shame. Many autistic people internalise their difficulties as ‘laziness’ or ‘lack of motivation’. The lack of real-time perception of fatigue does not mean it doesn’t exist. The fact that you can do something (capacity) does not mean it does not take an enormous toll on you (sustainability). The paradox of ‘high-functioning’ is explained here: people with high intellect are the most prone to severe burnout precisely because they have the cognitive ability to mask and override their body’s signals for long periods. They can ‘borrow’ energy from the future more efficiently, which leads to a greater energy debt and a more dramatic collapse. Burnout is, in this sense, proof that you have tried too hard, not too little.
Research-based recovery strategies
Radical Interoceptive Rest: Reducing demands and social withdrawal are an adaptive survival mechanism, not a pathological symptom. The individual must engage in rest that intentionally modulates the nervous system. Stimming as an interoceptive regulator: Repetitive behaviours (stimming), often discouraged by society, have proven to be vital interoceptive tools. They regulate the autonomic nervous system and generate clear signals that the brain can process easily. The Spoons Theory + The Forks Theory: Visual strategies for measuring limited energy (spoons) and the limit of sensory/social stressors (forks) in a day. Energy Accounting: Activities are recorded as withdrawals (which consume energy) or deposits (which provide energy). Recovery requires that deposits exceed withdrawals.
Skill Regression: Why can’t I do what I used to do?
One of the most terrifying traits of burnout is skill regression – the sudden inability to speak, cook, drive a car or plan the day. This is not a brain degeneration, but a strategic redistribution of energy. In a state of burnout, the brain goes into Survival Mode. Energy is withdrawn from ‘luxury’ or costly cortical functions (complex language, executive functions, impulse control) and redirected towards vital functions (breathing, temperature regulation, threat detection). You haven’t lost your intelligence; you’ve temporarily lost access to it because the ‘battery’ doesn’t have enough voltage to power those circuits. It is a biological defence mechanism: the system partially shuts down to prevent the battery from dying completely. Recovering energy will restore access to these abilities.
Recap: The Internal Mechanics of a Breakdown
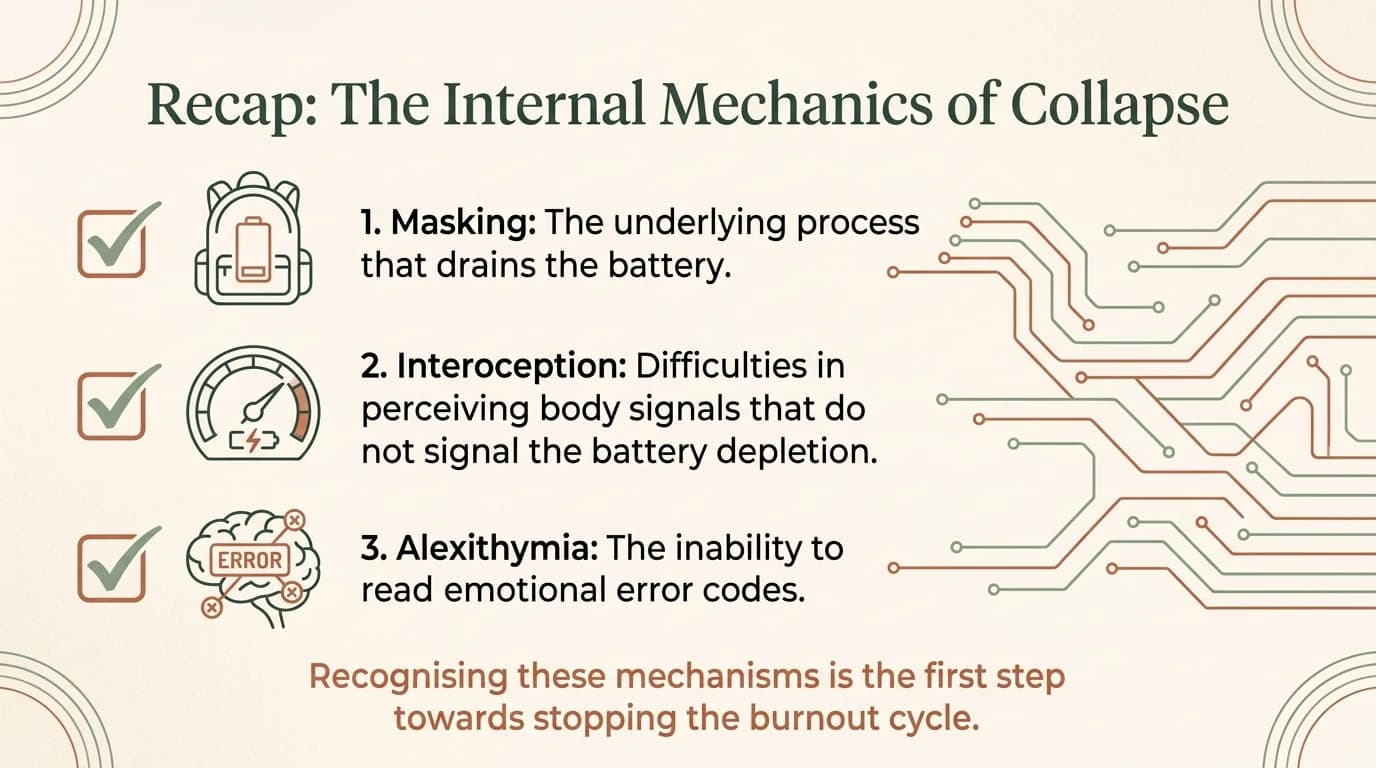
Before moving on to solutions, let’s consolidate our understanding of the three pillars. Masking is the active background process that drains resources. Interoception is the 8th sense, but in cases of neurodiversity it functions differently, providing a false perception of state sensors. Alexithymia is the difficulty in interpreting emotions and, by extension, in naming them. Recognising these mechanisms as biological and involuntary is the first therapeutic step. This shifts the discussion from “What’s wrong with me?” to “How can I adapt my environment and strategies to work with my nervous system, not against it?”. Awareness is the antidote to shame and the foundation of recovery.
The beginning of recovery from autistic burnout: Listening to the ‘whispers’
How do we reverse this process? Not through force, but through subtlety. Recovery begins by recalibrating the ability to listen to the body’s signals. We must learn to hear the body when it “whispers” (subtle signs of discomfort, mild irritability, tension in the shoulders), so as not to force it to “scream” (migraines, meltdowns, collapse). The three initial steps are:
- Awareness: Validating real needs through external monitoring (journals, alarms), if internal awareness is faulty.
- Safety: Creating ‘Safe Unmasking’ spaces, where the nervous system can let its guard down and stop the energy drain of masking.
- Pacing: Managing energy before it is completely depleted. Key message: The first step is not to do more, but to start listening to the silence between signals. Important note: Although the World Health Organisation (WHO) has officially recognised occupational burnout in the ICD-11, neither the ICD-11 nor the DSM-5-TR currently includes a diagnosis of autistic burnout. The lack of formal criteria maintains the risk of misdiagnosis with mood disorders or personality disorders. The provisional criteria proposed by Higgins et al. (2021) currently remain the best clinical basis.
What’s Next in Part 3
We have explored the internal mechanisms, but burnout does not occur in a vacuum. It is the result of the interaction between a vulnerable nervous system and a hostile environment. In the next part, we will explore the External Environment – the submerged part of the iceberg in the causality model. We will discuss sensory overload, systemic barriers, lack of accommodations, and the trauma of interacting with an unsupportive world. Stay tuned to complete the big picture and discover concrete strategies for adapting the environment to your needs (advocacy, sensory design), shifting responsibility from the individual to the context.
Are you ready to take the next step?
If what you’ve read resonates with you, you’re not alone. Neurodivergent burnout is a real experience, validated by research — and there are neuroaffirmative strategies that can help.
Book an Initial Consultation →
References
- Beck, J. S., et al. (2020). Camouflaging and mental health. Autism, 24(4), 809–821.
- Bird, G., & Cook, R. (2013). Mixed emotions: alexithymia and autism. Transl Psychiatry, 3(7), e285.
- Cassidy, S., et al. (2018). Risk markers for suicidality. Molecular Autism, 9, 42.
- DuBois, D., et al. (2016). Interoception in ASD. Int J Dev Neurosci, 53, 104–111.
- Higgins, J. et al. (2021). Defining autistic burnout through experts by lived experience. Autism in Adulthood.
- Hull, L., et al. (2017). Social Camouflaging in Adults with ASC. J Autism Dev Disord, 47(8), 2519–2534.
- Kinnaird, E., et al. (2019). Alexithymia in autism. European Psychiatry, 55, 80–89.
- Raymaker, D. M., et al. (2020). Defining Autistic Burnout. Autism in Adulthood, 2(2), 132–143.
- Walker, P. (2013). Complex PTSD: From Surviving to Thriving.
← The Anatomy of Burnout (Part 1) Sensory Overload (Part 3) →
Resources and support:
National Suicide Prevention Lifeline (US): 988 (call or text, 24/7)
Crisis Text Line: text HOME to 741741
Samaritans (UK): 116 123 (24/7)
Autism Society: autismsociety.org
CHADD (ADHD): chadd.org
New articles, directly to your inbox
Neuro-affirming content on ADHD, autism, AuDHD and PDA
— no spam, no aggressive frequency.

Explore interactive resources
More in this series

Next Steps
If this resonated, here are practical ways to go deeper.

