Therapy Without Masking: What It Should Feel Like When Therapy Actually Works
The cost of masking, sensory safety and how to recognise a neuro-affirming therapist. Red flags and green flags for neurodivergent people.

Who are the neurodivergent adults in therapy?
Adults who come to neuro-affirming therapy don't fit a single profile. Understanding their diversity is the first step toward an authentic approach.
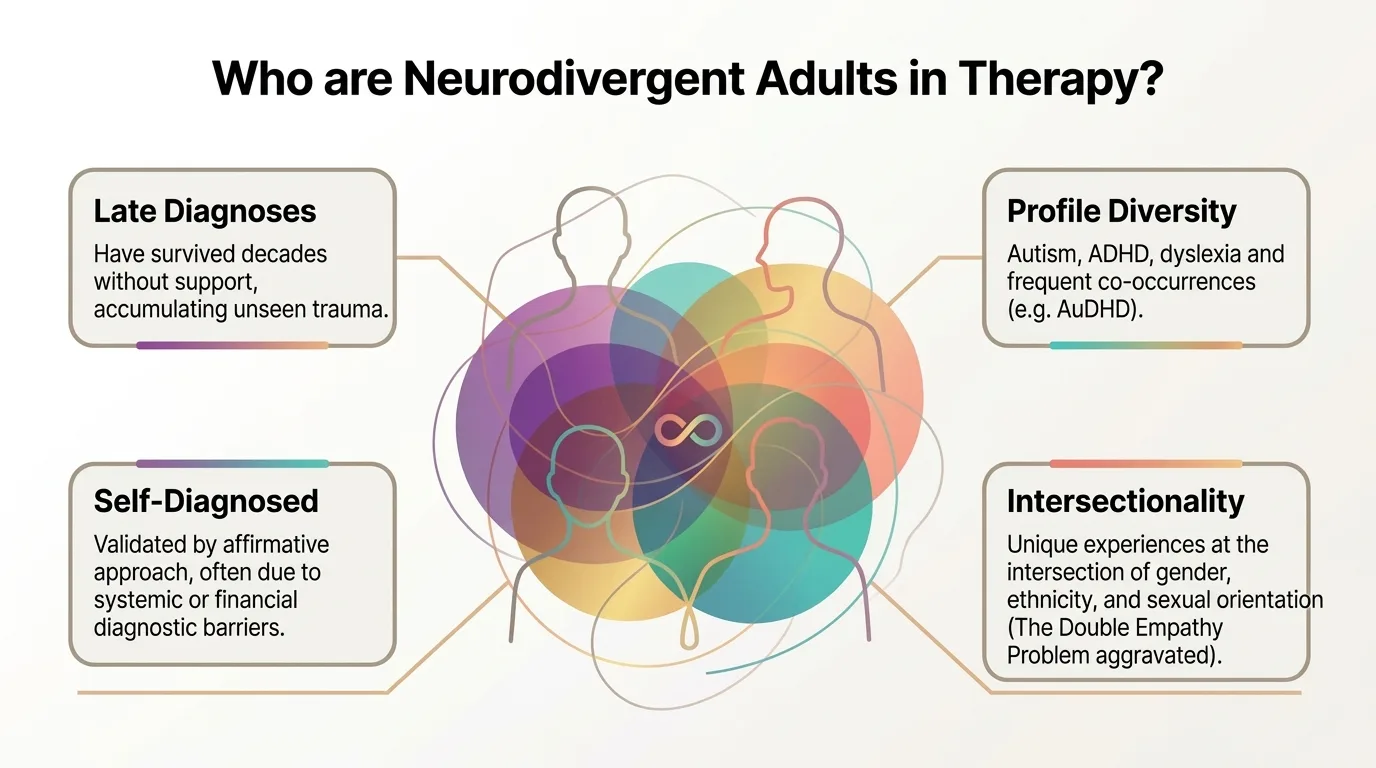
01 Profile Late Diagnoses They survived decades without support, accumulating invisible trauma. Many people receive their autism or ADHD diagnosis only at 30, 40, or 50 — after a lifetime of adaptation effort without understanding why everything seems harder.
02 Profile Profile Diversity Autism, ADHD, dyslexia, and frequent co-occurrences (e.g., AuDHD — autism + ADHD simultaneously). Each combination creates a unique profile of needs and strengths.
03 Profile Self-Identified Long waiting lists, prohibitive costs, clinician bias against women and people of colour, and assessment tools normed on white boys all create systemic barriers to formal diagnosis. Self-identification is clinically valid (Doherty et al., 2022) and the affirmative approach honours it fully.
04 Profile Intersectionality Unique experiences at the intersection with gender, ethnicity, and sexual orientation. The 'Double Empathy Problem' is often compounded by these additional dimensions of marginalization.
· · ·
Chronic invalidation and the cost of masking
For many neurodivergent adults, repeated experiences of invalidation during childhood build a deeply negative self-image. When, for years, you are told — verbally or non-verbally — that the way you exist is "too much" or "not enough", you internalise those messages. They become the lens through which you see yourself and the world around you.
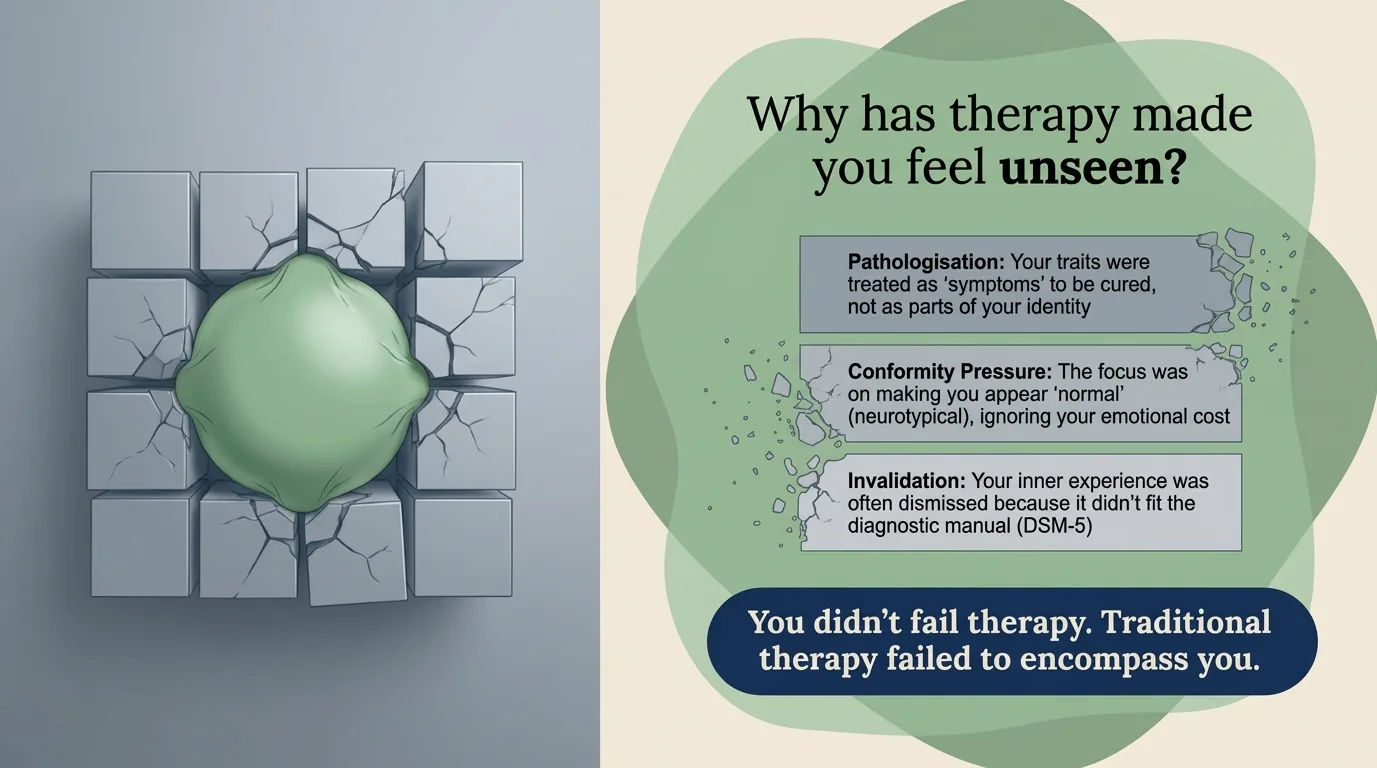
Infographic: Why traditional therapy made you feel unseen — pathologising, pressure, invalidation This chronic invalidation takes many forms:
Forms of chronic invalidation
Constant comparisons with siblings or classmates: "Why can't you be more like your sister?" Relentless negative feedback at school: "They could do so much more if they just focused" Relationships where you are permanently "the difficult one" or "the sensitive one" Previous therapy experiences that deepened the feeling of being misunderstood Late diagnoses that come with the grief of having been misjudged for years
Masking: survival at an invisible cost
The natural response to chronic invalidation is masking (also called camouflaging) — the conscious or automatic effort to suppress neurodivergent traits and mimic neurotypical behaviour. As Roisenberg (2025) emphasises, it is not a choice — it is a survival strategy developed from childhood.
Research (Hull et al., 2017; Cook et al., 2021) identifies three main masking strategies:
01 Strategy 1 Compensation Developing elaborate strategies to offset difficulties: memorised social scripts, forced eye contact, mirroring other people's facial expressions.
02 Strategy 2 Suppression Actively inhibiting authentic behaviours: stopping stimming, suppressing sensory reactions, hiding special interests.
03 Strategy 3 Assimilation Full integration into the neurotypical environment, to the point of losing contact with the authentic self — "Who am I, really, without the mask?"
Infographic: The masking cascade — from conformity pressure to neurodivergent burnout Masking consumes enormous cognitive resources. It is the equivalent of running an autopilot system manually, all the time: every social interaction requires conscious processing, monitoring, adjusting. Every forced smile, every deliberately maintained eye contact, every suppressed reaction — all of it draws from your daily cognitive budget.
Over time, this effort leads to neurodivergent burnout — a profound exhaustion that Raymaker et al. (2020) define as "having all of your internal resources exhausted beyond measure" — one that cannot be resolved by "a holiday" or "some rest", because its source persists. Kupferstein's (2018) study showed that 46% of individuals exposed to compliance-based therapies (ABA) met the criteria for PTSD.
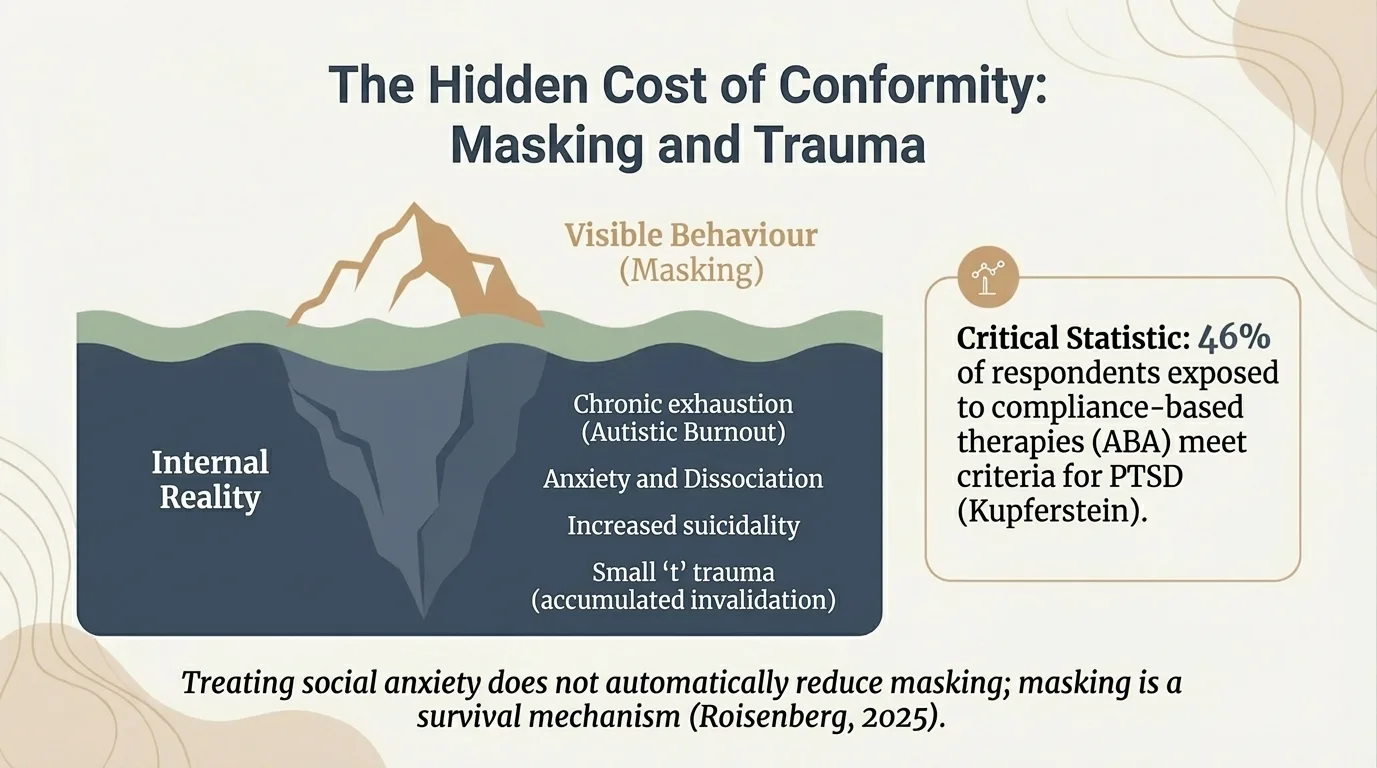
Infographic: The masking iceberg — what is visible on the surface vs. what happens inside
"Masking is not politeness. It is a survival mechanism that drains the cognitive resources that should have been available for your actual life."
The scientific evidence of the cost
Bradley et al. (2021) studied 277 autistic adults and discovered that the time spent camouflaging is the most destructive factor for mental health. Participants described masking as necessary for survival, but the price paid was isolation, unrealistic perceptions from others, and physical and mental deterioration. Hull et al. (2021) demonstrated that masking strongly predicts generalized and social anxiety — being a major risk factor independent of gender. Compensatory strategies — mental rehearsal of conversations, forced control of eye contact — are fundamentally unsustainable (Livingston et al., 2019). They fail in moments of stress, exactly when the person needs them most. Pearson and Rose (2021) emphasize that masking is 'the illusion of choice' — driven by fear of rejection, not a desire for conformity. Therapies that encourage masking erode trust and worsen trauma, rather than healing it. Cage and Troxell-Whitman (2019) demonstrated the direct link between masking pressure and increased rates of depression, self-alienation, and suicidal ideation.
This is precisely why, before any psychological exploration, a foundation must be built that most traditional approaches overlook entirely.
· · ·
The invisible foundation: sensory safety
Before any deep psychological exploration can begin, a foundation must be laid that most therapists overlook: sensory safety. Without it, traditional cognitive therapy (talk-based processing) is completely ineffective.
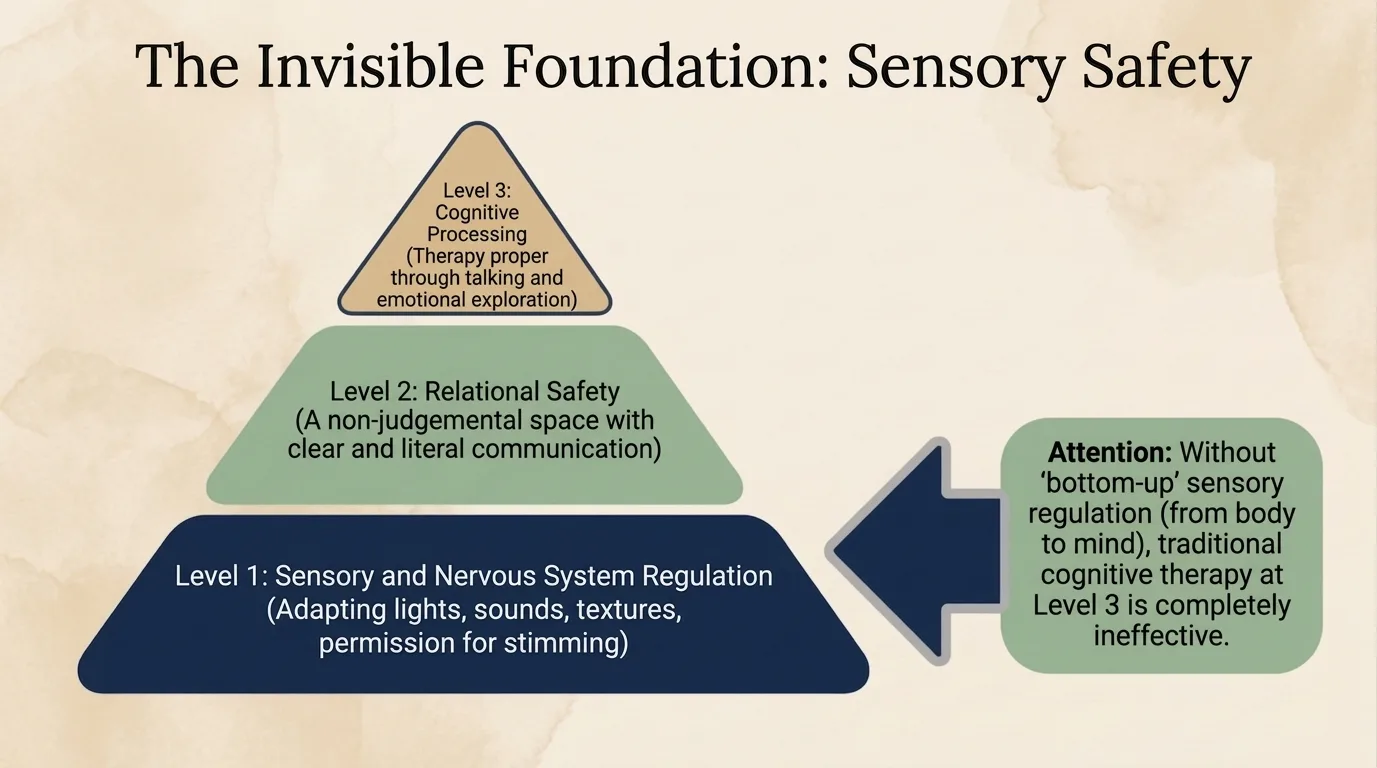
Infographic: The Sensory Safety Pyramid — without the sensory base, the upper levels cannot function The pyramid works like this:
1 Level 1 Sensory Regulation Adjusting lights, sounds, textures. Permission for stimming. Without bottom-up sensory regulation (from body to mind), nothing else works.
2 Level 2 Relational Safety A space free of judgement, with clear and literal communication. The client needs to feel they can be authentic without consequences — otherwise masking continues into the therapy room itself.
3 Level 3 Cognitive Processing Only here — actual talk therapy and emotional exploration. Most therapists skip straight to this level, ignoring the foundation underneath.
Note: Without bottom-up sensory regulation (from body to mind), traditional cognitive therapy at Level 3 is completely ineffective. It is like trying to run complex software on a computer that is overheating — you fix the hardware first.
Felt safety and alexithymia
Fuld and McKelvie (2024) introduce the concept of 'felt safety' as the foundation of the neuro-affirmative therapeutic relationship. It is not enough for the environment to be objectively safe — the client's nervous system must feel safety through predictability, validation, and the absence of masking pressure.
· · ·
What a neuro-affirming session looks like
One of the most common questions I get is: "But practically, what does it look like?" Here are the concrete adaptations that make the difference:
Session Adaptations 1 Camera off is fine. If you process better without the visual stimulation of someone's face, you can keep your camera off. We work 100% online, and the format adapts to your sensory needs.
2 Stimming is welcome. Fidget toys, repetitive movements, pacing around the room — these are all forms of sensory regulation, not distractions. You will never be asked "why are you doing that".
3 Text-based communication when needed. Sometimes spoken words are inaccessible — especially during sensory overload or shutdown. You can type in the chat, send a message after the session, or bring written notes.
4 Built-in sensory breaks. If you feel overwhelmed, we pause. You do not have to explain. You do not have to "push through". We respect the signals from your nervous system.
5 Processing time is respected. Silence is not a sign of "resistance". If you need 30 seconds or 3 minutes to process a question, that time is yours. I will not fill the silence with words.
6 Direct communication, no ambiguity. Questions are clear and concrete. Feedback is explicit, not implied. I do not use vague language or "reading between the lines" — because I know from experience how exhausting it is to decode.
7 Flexibility for PDA (Pathological Demand Avoidance). If direct demands trigger avoidance, we work with options, not directives. "We could explore..." instead of "You need to...".
I am autistic and ADHD myself. Every adaptation in the list above does not come from theory — it comes from the experience of being a neurodivergent client in therapy that was not built for me. I know how it feels. And that is why I do things differently.
· · ·
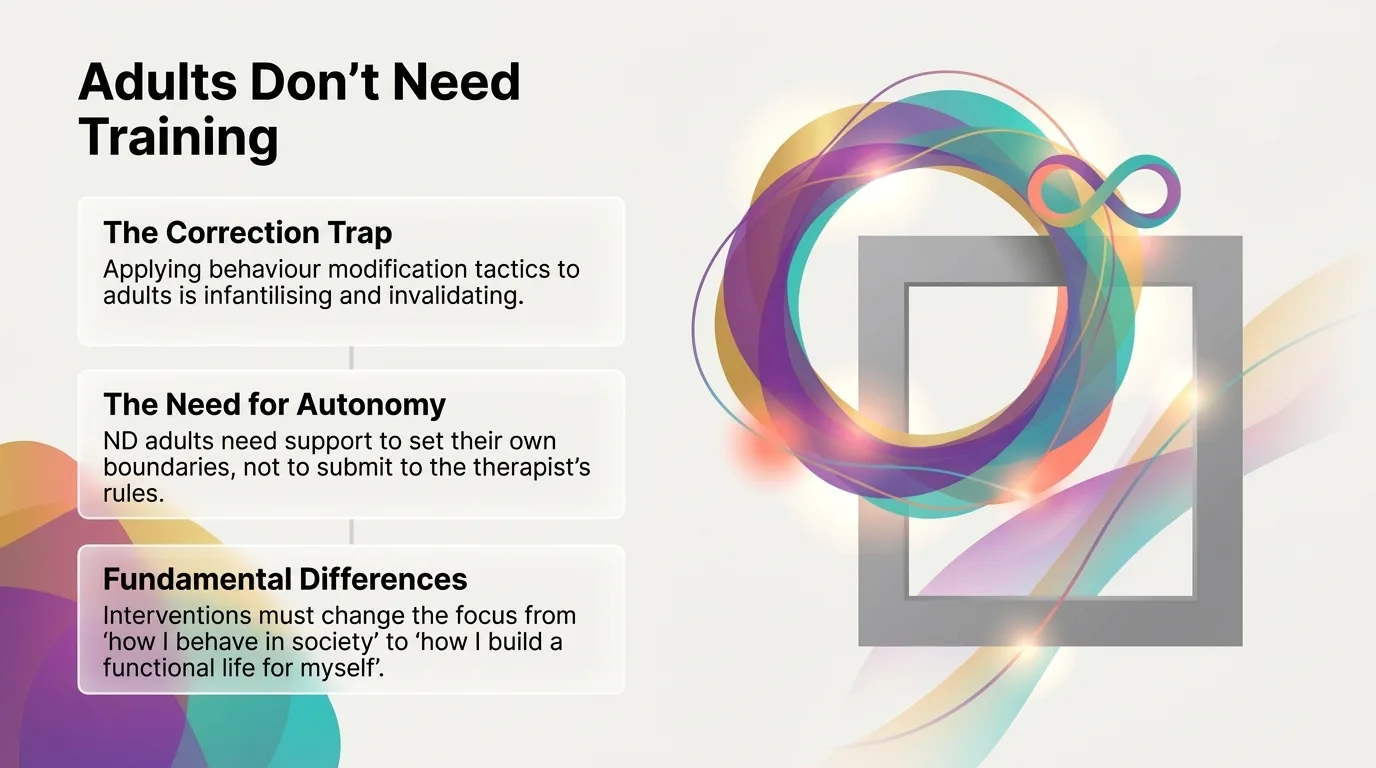
The integrative approach: mind and body as a whole
I do not work with the "mind" alone — I work with the entire system. Mental health is deeply connected to physical, emotional and sensory wellbeing. This integrative perspective is especially essential for neurodivergent adults, whose emotional experiences often manifest directly in the body.
Infographic: Interoception — the internal sense that explains why burnout seems to appear "out of nowhere"
Interoception: the 8th sense
Interoception — the ability to perceive the body's internal signals (hunger, fatigue, pain, stress) — works differently in the neurodivergent brain (Price & Hooven, 2018). Many autistic and ADHD adults struggle to recognise their own internal states, which leads to a profound disconnection from their own body.
In practical terms, this means: you do not feel that you are exhausted until you crash. You do not feel hunger until you are shaking. You do not recognise stress until it turns into panic or shutdown. In therapy, we actively work on reconnecting with these signals — not forcefully, but gradually, respecting your pace.
Polyvagal Theory and regulation
Polyvagal Theory (Porges, 2011) helps us understand why the neurodivergent nervous system often oscillates between hyperactivation (anxiety, overstimulation, meltdown) and hypoactivation (shutdown, freeze, dissociation). It is not a "problem with emotional control" — it is biology.
In sessions, we integrate somatic (body-based) techniques that support regulation:
Somatic tools used
Adapted breathing exercises — not the "standard" 4-7-8 breathing that can actually increase anxiety in some neurodivergent people, but variations that work with your sensory profile Gradual body awareness — reconnecting with interoceptive (body) signals at a pace that does not overwhelm Sensory grounding — using your preferred (not imposed) sensory stimuli for anchoring Energy rhythm tracking — identifying your natural rhythms of activation and rest, for sustainable energy management
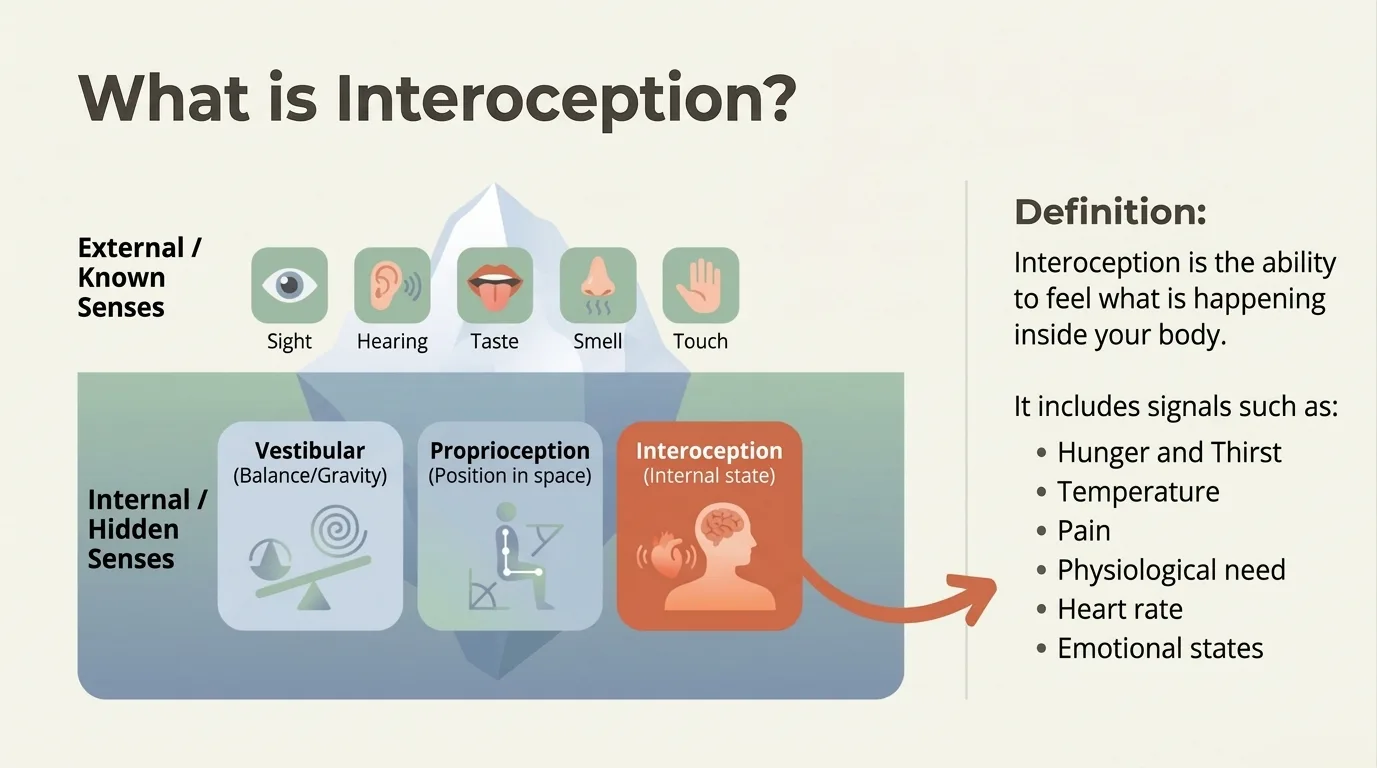
Infographic: What is interoception — the hidden senses beyond the 5 we all know
IFS: the internal parts system
One of the approaches I frequently integrate is Internal Family Systems (IFS) (Schwartz, 2021) — a model that understands the mind as a system of internal parts, each with its own role and history. For neurodivergent adults, IFS is often the first therapeutic model where their inner experience finally makes sense, rather than feeling chaotic.
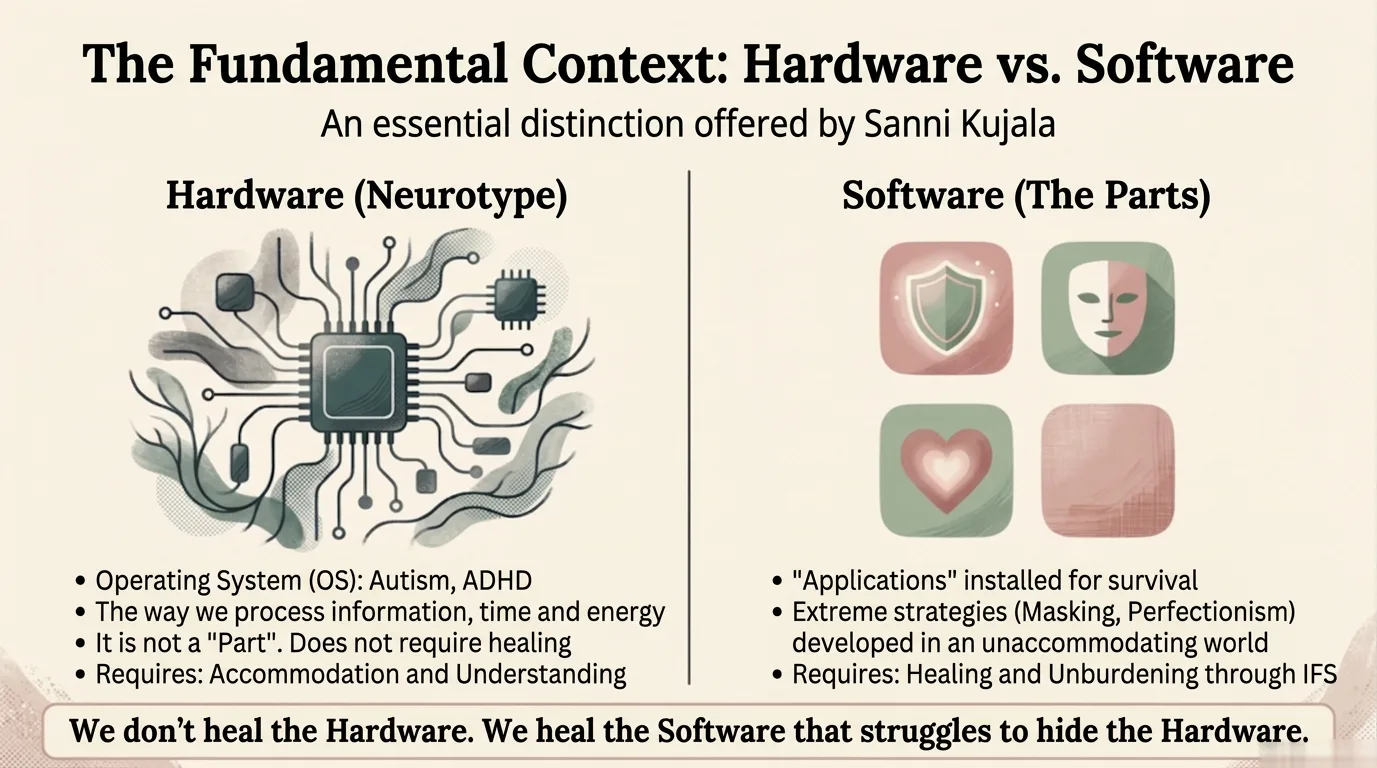
Infographic: IFS — we do not "fix" the neurodivergent brain, we heal the survival strategies The part that withdraws before a difficult conversation. The part that pushes forward without stopping, even when exhaustion is total. The part that masks at work and cannot stop masking at home either. IFS works with all of them — with curiosity, not confrontation.
Clinical evidence for specific approaches
Neuro-Affirmative DBT Group Dialectical Behavior Therapy Halmøy et al. (2022) demonstrated that group Dialectical Behavior Therapy, applied from a neuro-affirmative perspective, significantly improves executive functions, emotional regulation, and quality of life in adults with ADHD.
ACT + Psychoeducation Acceptance and Commitment Therapy Seery et al. (2023) showed that Acceptance and Commitment Therapy, combined with psychoeducation, increases self-understanding, self-acceptance, and self-compassion in adults with ADHD, gradually eliminating internalized shame.
Adapted Mindfulness Active and Movement-Based Mindfulness Haydicky et al. (2013) discovered that standard mindfulness techniques (passive, stillness-based) often fail for the neurodivergent brain. Instead, active or movement-based mindfulness leads to significant reductions in depression and anxiety.
· · ·
Red flags and green flags: how to spot a good-fit therapist
Choosing a therapist is one of the most important decisions you can make. And for a neurodivergent person, the stakes are even higher — a poor-fit therapist does not just fail to help, they can cause real harm. Here are the signs to watch for:
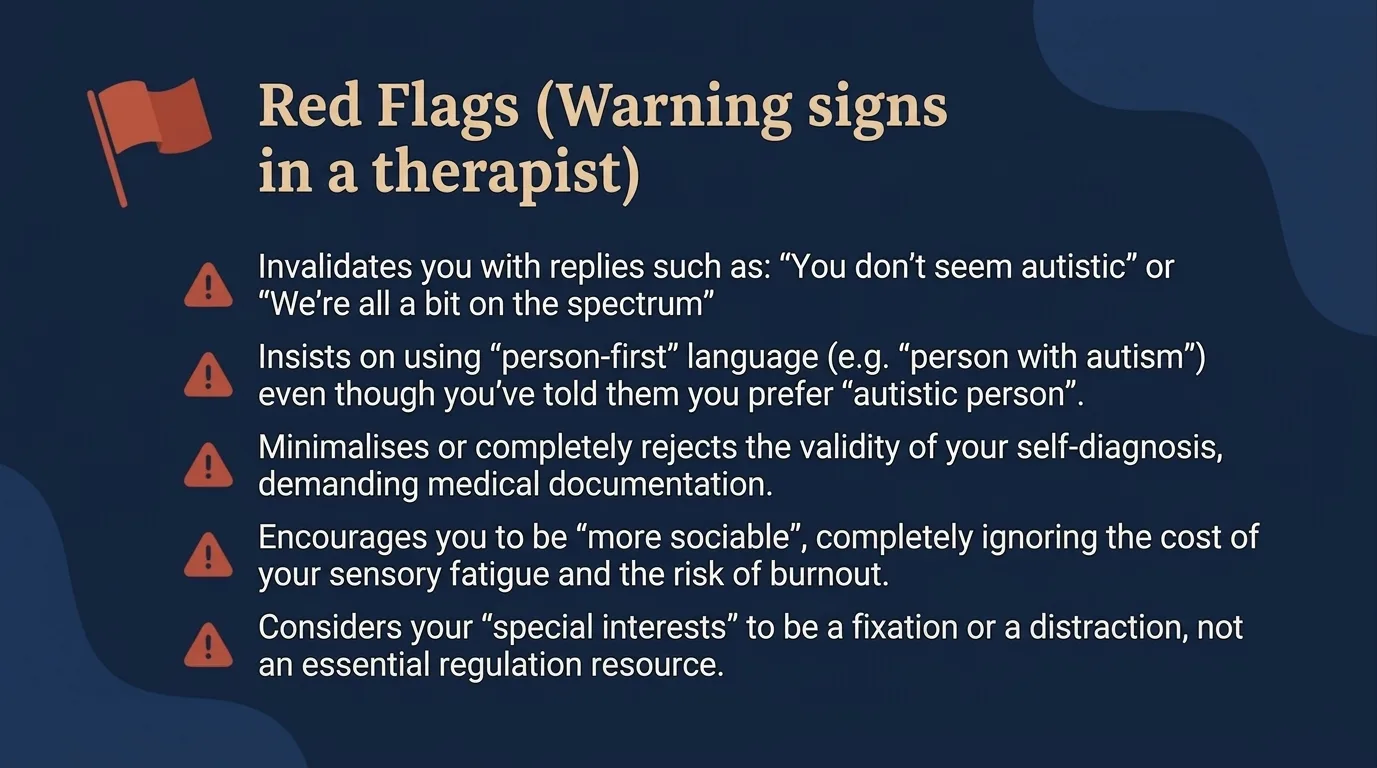
Infographic: 5 warning signs that a therapist is not neuro-affirming
Red Flags
- They invalidate you: "You don't look autistic" or "We're all a little on the spectrum"
- They insist on "person-first" language even though you prefer "autistic person"
- They dismiss or minimise your self-diagnosis
- They encourage you to be "more sociable", ignoring the sensory cost
- They consider special interests a "fixation" or "distraction"
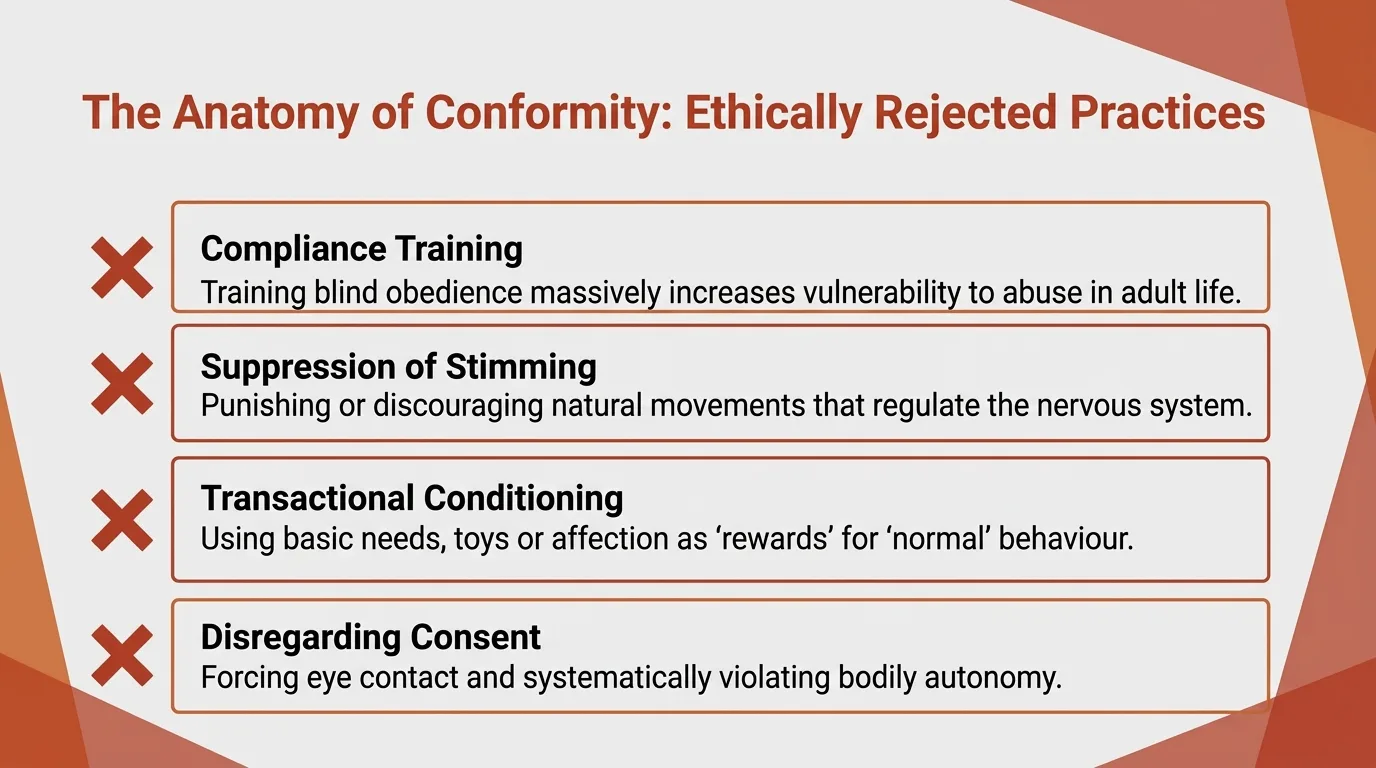
- They want to eliminate stimming or "repetitive behaviours"
- They encourage 'compensatory strategies' or 'social skills training' without acknowledging the cost of masking
- They do not know or dismiss the concept of spiky profile Green Flags
- They respect and use special interests (monotropism) as a resource
- They offer physical accommodations proactively: adjust lighting, accept fidgeting
- They communicate directly and literally, checking they have understood you correctly
- They validate self-diagnosis as equally real and valid as a clinical one
- They allow bodily autonomy: you can move, no forced eye contact
- They understand the difference between neurodivergent burnout and depression
- They know and apply the concept of 'felt safety' — adapting both the physical and relational environment
- They recognise the validity of self-diagnosis and do not condition therapy on a formal diagnosis
- They use adapted therapeutic tools (active mindfulness, modified DBT, ACT with psychoeducation)
You are a client hiring a service. You have every right to ask questions in the first session to protect your energy: "What is your view on the neurodiversity paradigm?" "How do you approach autistic burnout?" "Are you willing to offer accommodations in sessions?"
· · ·
Is this approach right for you?
This approach is for you if:
You have been diagnosed as neurodivergent (autism, ADHD, AuDHD, PDA, dyslexia, dyscalculia, OCD) or suspect that you are You have been through therapies where you felt invalidated, judged, or treated as a project to be "fixed" You are looking for a space where you no longer have to explain why certain things that are "simple" for others are overwhelming for you You are experiencing neurodivergent burnout and need a therapist who understands the difference from depression You want to work with someone who has lived experience, not just theoretical knowledge, of neurodivergence You understand that different does not mean defective — and you are looking for a therapist who starts from the same premise
If you recognise yourself in what you have read above and want to explore what a therapeutic space built around your real needs — not other people's expectations — could look like, I invite you to a first conversation.
References
- Bradley, L., Shaw, R., Baron-Cohen, S., & Cassidy, S. (2021). Autistic adults' experiences of camouflaging and its perceived impact on mental health. Autism in Adulthood, 3(4), 320-329.
- Cage, E. & Troxell-Whitman, Z. (2019). Understanding the reasons, contexts and costs of camouflaging for autistic adults. Journal of Autism and Developmental Disorders, 49(5), 1899-1911.
- Cook, J., Crane, L., Bourne, L., et al. (2021). Camouflaging in autism: A systematic review. Clinical Psychology Review, 89, 102080.
- Doherty, M., Neilson, S., O'Sullivan, J., et al. (2022). Barriers to healthcare and self-reported adverse outcomes for autistic adults: A cross-sectional study. BMJ Open, 12(2), e056904.
- Fuld, S. & McKelvie, A. (2024). Felt safety as foundation: A neuro-affirmative framework for therapeutic practice. Autism, 28(3), 612-625.
- Halmøy, A., Ring, A.E., Gjestad, R., & Møller, M. (2022). Dialectical behaviour therapy-based group treatment for adults with ADHD: A feasibility study. Nordic Journal of Psychiatry, 76(4), 273-281.
- Haydicky, J., Shecter, C., Wiener, J., & Ducharme, J.M. (2013). Evaluation of MBCT for adolescents with ADHD and their parents: Impact on individual and family functioning. Journal of Child and Family Studies, 24(1), 76-94.
- Hull, L., Levy, L., Lai, M.C., et al. (2021). Is social camouflaging associated with anxiety and depression in autistic adults? Molecular Autism, 12(1), 13.
- Hull, L., Petrides, K.V., Allison, C., et al. (2017). "Putting on my best normal": Social camouflaging in adults with autism spectrum conditions. Journal of Autism and Developmental Disorders, 47(8), 2519-2534.
- Kupferstein, H. (2018). Evidence of increased PTSD symptoms in autistics exposed to applied behavior analysis. Advances in Autism, 4(1), 19-29.
- Livingston, L.A., Shah, P., & Happé, F. (2019). Compensatory strategies below the behavioural surface in autism: A qualitative study. Molecular Autism, 10(1), 47.
- Mul, C.L., Stagg, S.D., Herbelin, B., & Aspell, J.E. (2018). The feeling of me feeling for you: Interoception, alexithymia and empathy in autism. Journal of Autism and Developmental Disorders, 48(9), 2953-2967.
- Pearson, A. & Rose, K. (2021). A conceptual analysis of autistic masking: Understanding the narrative of stigma and the illusion of choice. Autism in Adulthood, 3(1), 52-60.
- Porges, S.W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W.W. Norton.
- Price, C.J. & Hooven, C. (2018). Interoceptive awareness skills for emotion regulation: Theory and approach of Mindful Awareness in Body-Oriented Therapy (MABT). Frontiers in Psychology, 9, 798.
- Raymaker, D.M., Teo, A.R., Steckler, N.A., et al. (2020). "Having all of your internal resources exhausted beyond measure and being left with no clean-up crew": Defining autistic burnout. Autism in Adulthood, 2(2), 132-143.
- Roisenberg, L. (2025). Neurodivergent masking as a survival strategy: Clinical implications for therapy. Journal of Neurodiversity in Clinical Practice, 3(1), 45-62.
- Schwartz, R.C. (2021). No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model. Sounds True.
- Seery, C., Sharry, J., &Onal, S. (2023). ACT-based psychoeducation for ADHD in adults: A qualitative study. Journal of Contextual Behavioral Science, 28, 127-136.

Next Steps
If this resonated, here are practical ways to go deeper.