The Anatomy of Neurodivergent Burnout — Part 1
Why does neurodivergent burnout look like depression — but require the opposite treatment? A neuroaffirmative, research-based guide.
If this sentence resonates with you, here is a possibility that few specialists consider: you may not be dealing (only) with classic clinical depression, but with Autistic Burnout, a distinct phenomenon that requires an almost diametrically opposite approach.
More often than not, neurodivergent people end up in a specialist’s office reporting chronic fatigue and a loss of interest in their current activities and responsibilities. The standard diagnosis? Depression. The standard treatment? Antidepressants and the endless encouragement to “Be active, get out of the house, exercise, socialise” – in other words, Behavioural Activation.
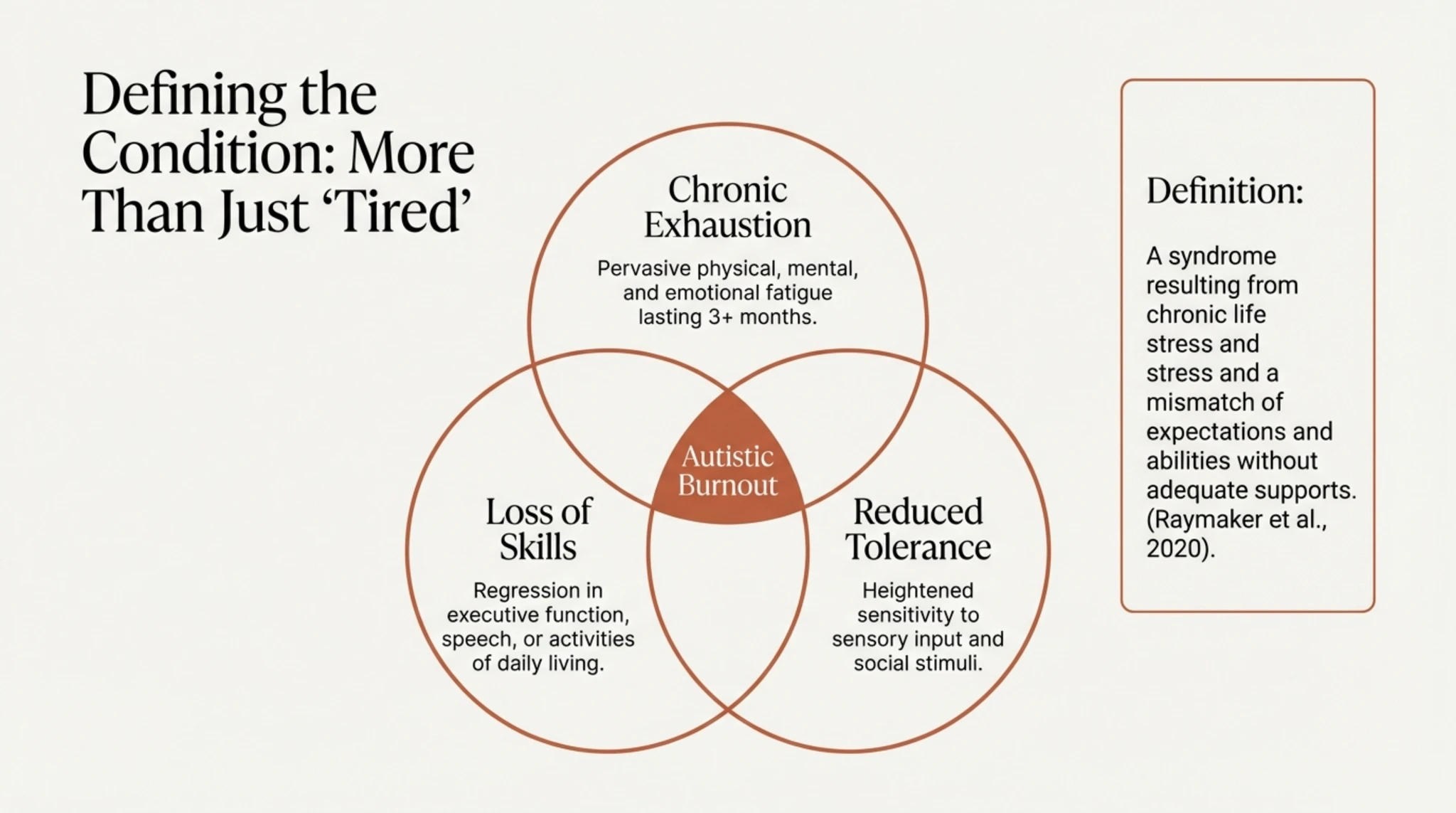
According to the landmark research by Raymaker et al. (2020), Autistic Burnout is defined as: “A syndrome resulting from chronic stress and an imbalance between expectations and abilities, in the absence of adequate support. It is characterised by generalised exhaustion, loss of function and reduced tolerance to stimuli.”
And here is the critical difference: Raymaker et al. demonstrated that Autistic Burnout is distinct from clinical depression, with a completely different aetiology and presentation.
This is the first part of a mini-series of posts dedicated to raising awareness of Autistic Burnout. In these slides, we explore:
What is Autistic Burnout, Actually? The critical difference between “I don’t want to/It’s pointless” (Depression) and “I want to, but I can’t” (Burnout) Why standard approaches to depression can do more harm than good when applied during burnout The invisible mechanisms: Masking and Interoception
———
The Anatomy of Neurodivergent Burnout
This presentation opens the discussion on a common, yet often misunderstood, experience within the neurodivergent community: exhaustion or burnout. Unlike ordinary tiredness, we are talking here about a complex physiological and neurological phenomenon, analysed through the lens of recent research, including the work of Dr Megan Anna Neff and the AASPIRE studies coordinated by Dora Raymaker.
My aim is to move beyond the myths and understand the biological mechanisms behind the ‘crash’ that many experience after years of forced adaptation. In the following slides, we will explore why standard recovery strategies often fail and how the science behind burnout can offer us a real roadmap to stability, validating the lived experience of those who feel they ‘can’t go on’.
———
What is Autistic Burnout?
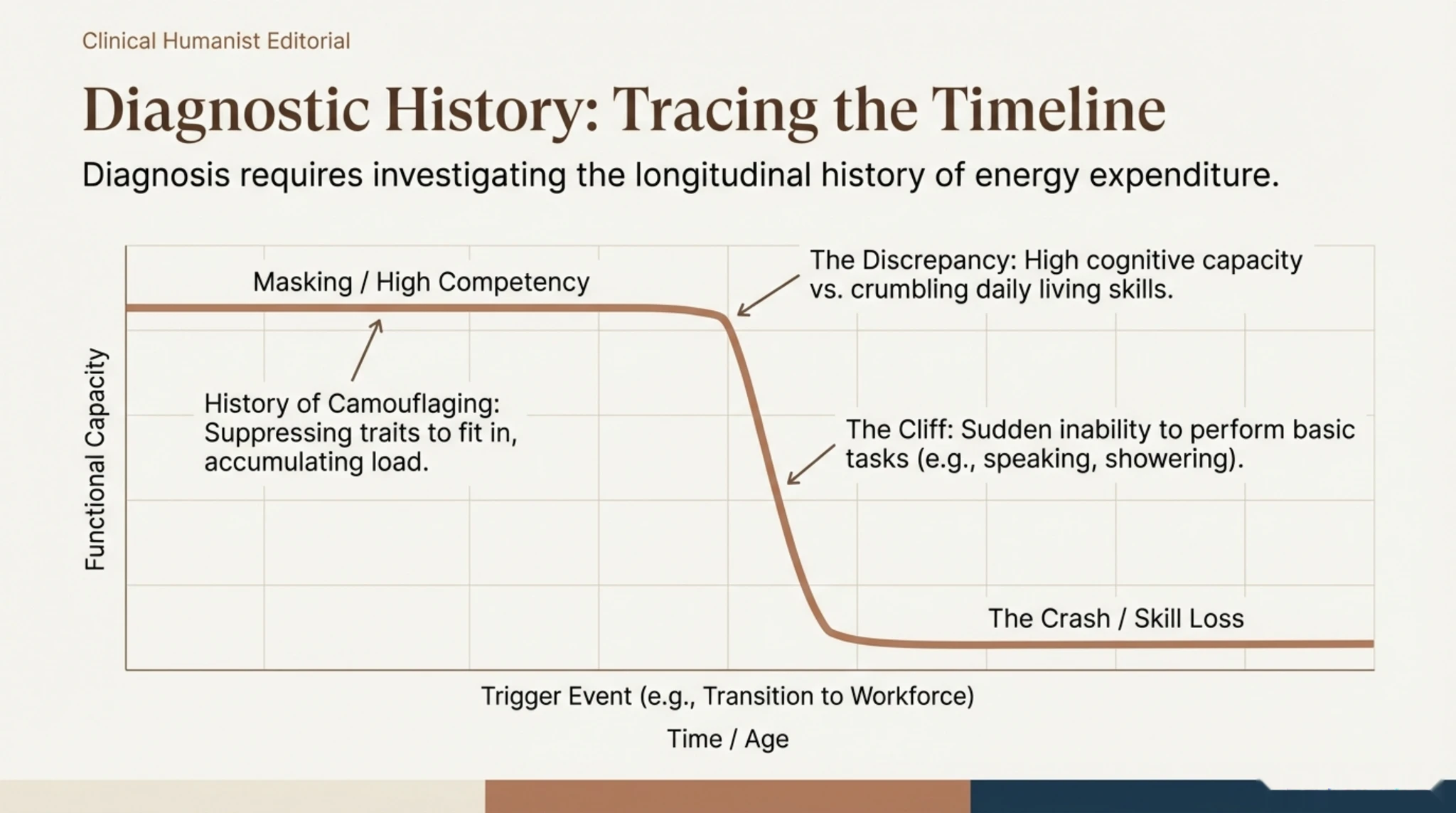
Academic studies, particularly those by Raymaker et al. (2020), define autistic burnout through a specific triad of symptoms that distinguishes it from classic occupational burnout: extreme chronic exhaustion, loss of acquired skills (such as speech or self-care), and a dramatically reduced sensory tolerance. This is metaphorically described as a state in which ‘all internal resources have been exhausted beyond measure, leaving no “clean-up crew” to repair the damage’.
This state is not the result of a single bad day, but the accumulation of long-term chronic stress, caused by navigating a world that is not built for neurodiversity. At this stage, the person not only feels exhausted but experiences a functional regression; tasks that were once simple become impossible, and sensory stimuli that were tolerable suddenly become painful, signalling that the nervous system is in survival mode.
New Research Findings (2024–2026)
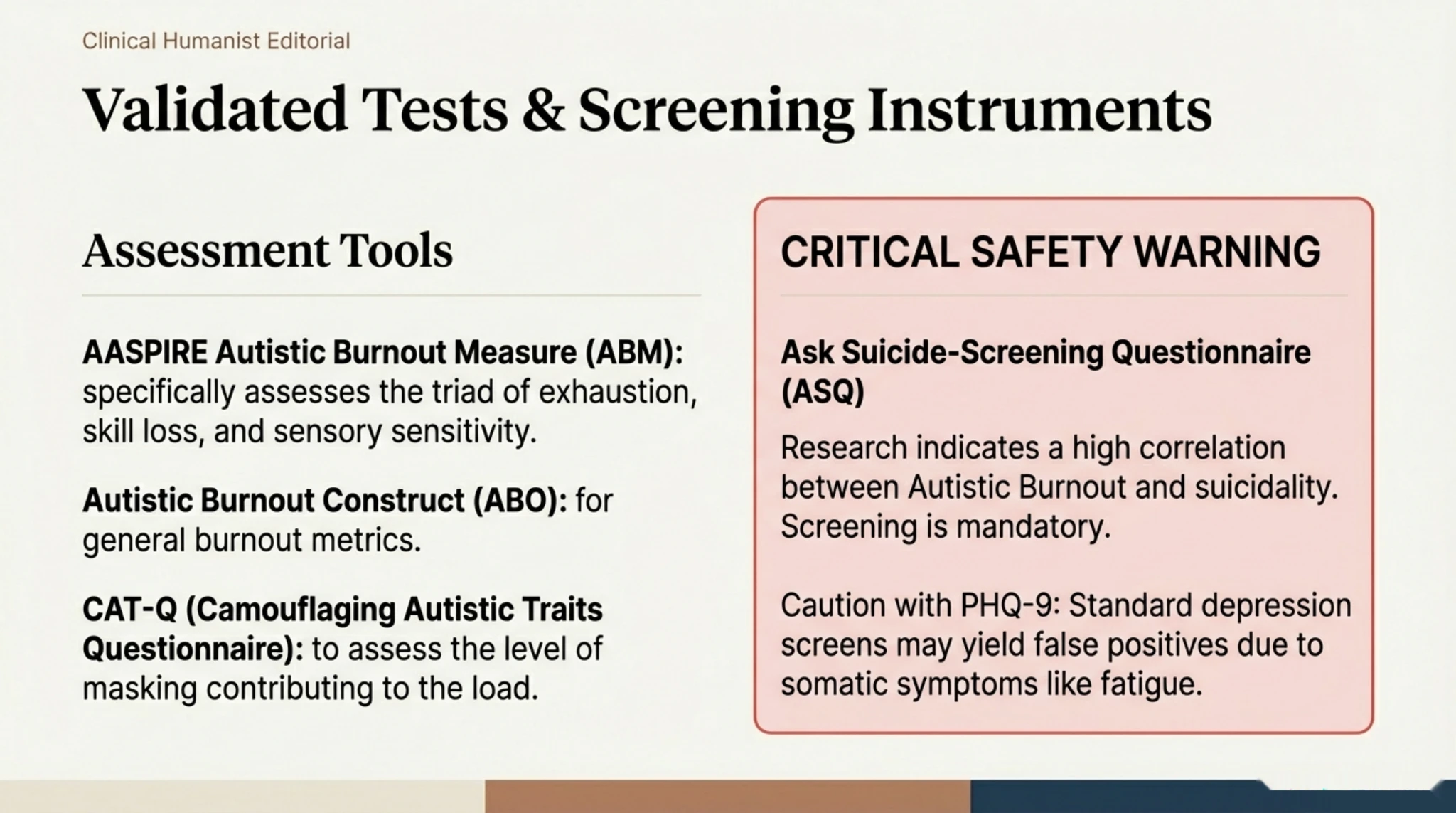
69% of autistic people have experienced autistic burnout (Mantzalas et al., 2024) 46% have had 4 or more episodes of burnout over the course of their lives Meta-analysis (Ali et al., 2025): 48 studies, ~4,000 participants — autistic burnout may be chronic with intermittent episodes, not an isolated event The AASPIRE Autistic Burnout Measure (ABM) has been psychometrically validated (Bougoure et al., 2025): excellent internal consistency (ω = 0.98), effectively distinguishes individuals experiencing burnout (AUC = 0.92)
———
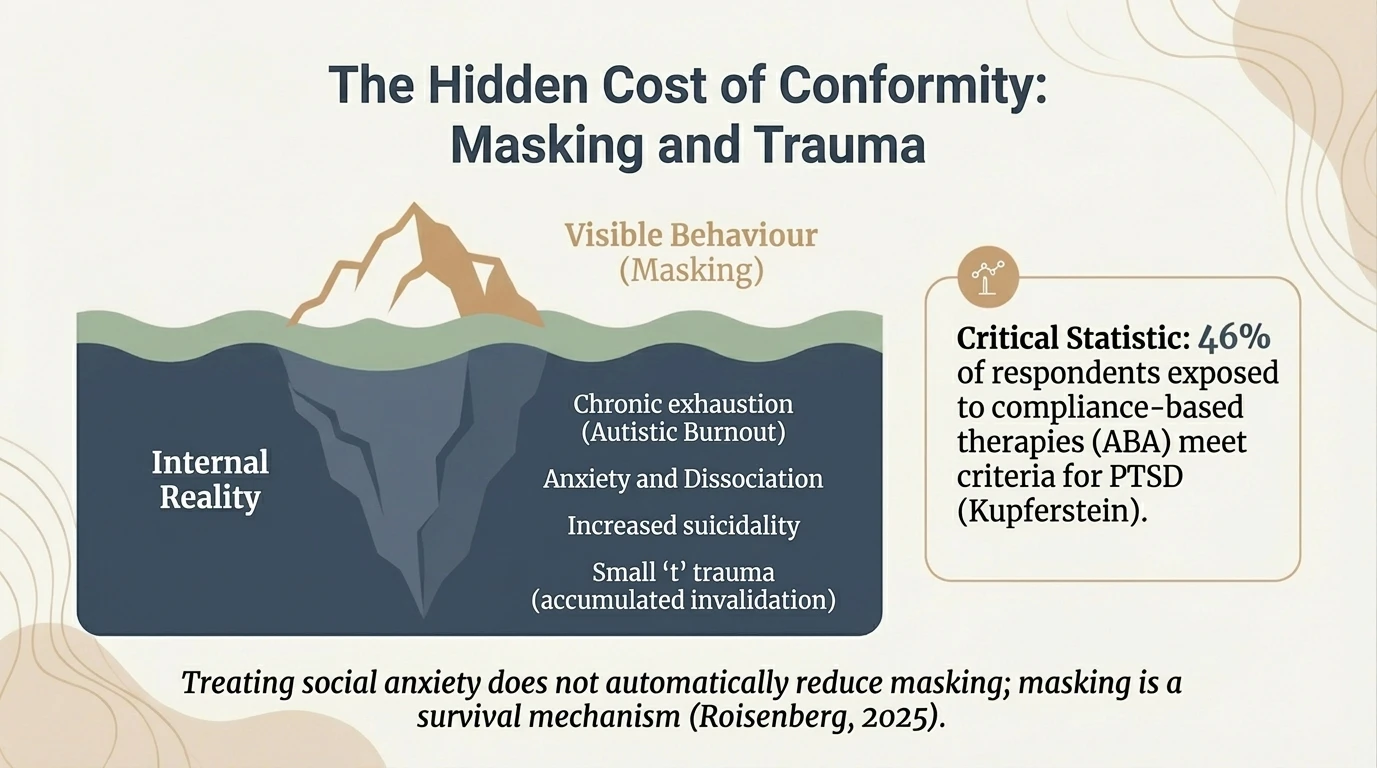
The Iceberg Model
To understand why burnout occurs, we need to look below the ‘waterline’, using the iceberg model. What we see on the surface — seemingly normal functioning or even high performance — is underpinned by massive cognitive and energetic costs. These invisible causes include constant masking (concealing autistic traits), the effort to manage systemic barriers, unforeseen changes, and constant sensory overload.
The crucial message of this slide is the externalisation of blame: exhaustion is not a personal failure or a lack of resilience, but the direct result of a hostile or unsuitable environment. When a neurodivergent person has to process social interactions ‘manually’ and consciously filter out the background noise that others automatically ignore, their internal battery drains at an accelerated rate, inevitably leading to a breakdown if there is no adequate support.
———
Key distinction: Ability vs. Motivation
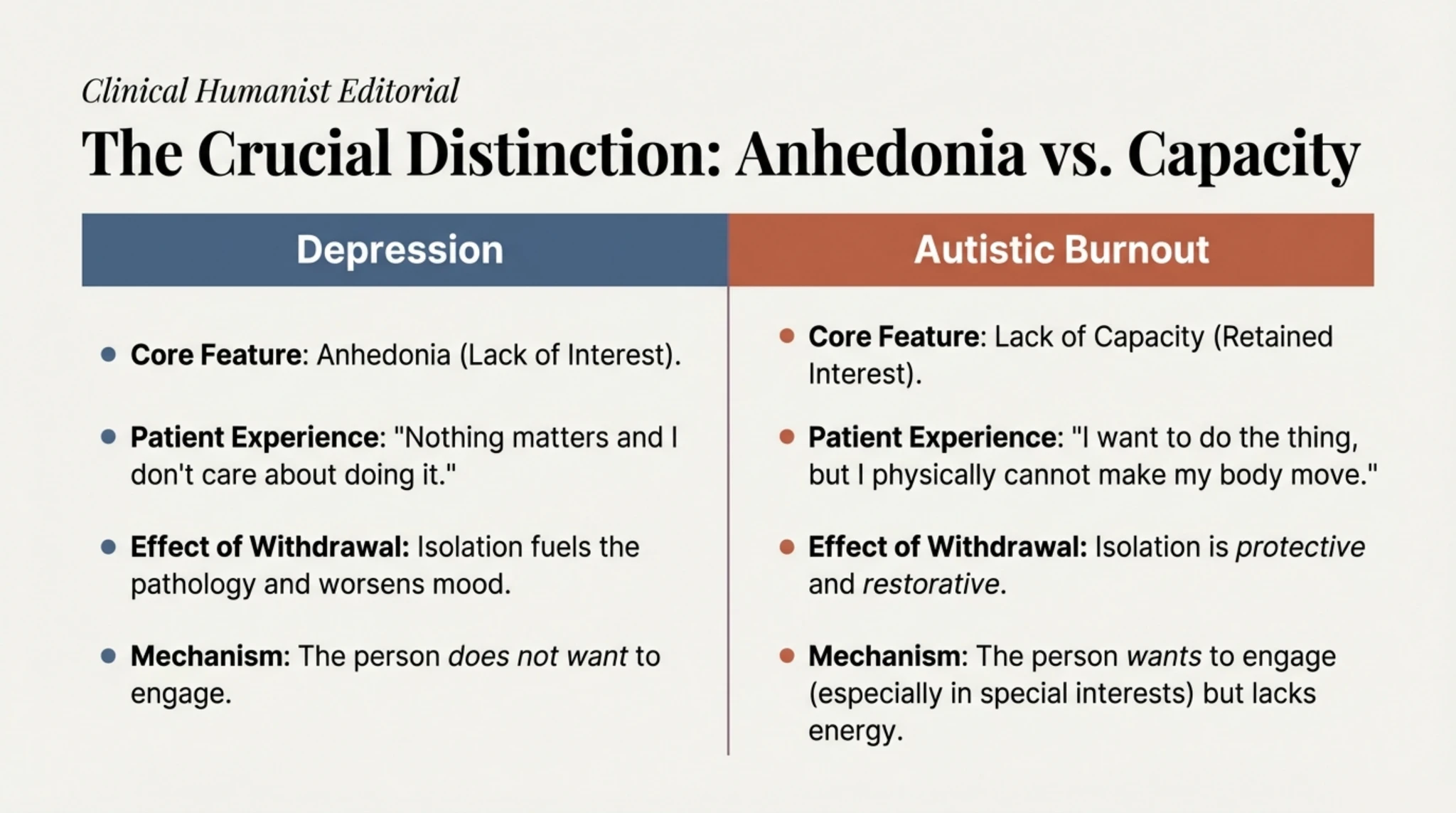
This distinction is perhaps the most important differential diagnostic tool at our disposal. In classic clinical depression, inactivity is primarily driven by anhedonia — the inability to feel pleasure — which translates into a “I don’t want to” or “I don’t care”. The depressed person stops painting, socialising or working because these activities no longer offer any emotional reward.
Internal motivation has vanished, giving way to apathy and a sense of hopelessness. In contrast, in neurodivergent burnout, we face a crisis of capacity, defined by “I want to, but I can’t”. The person experiencing burnout often retains the desire and passion for their interests — they would desperately like to get started on that creative project or reply to that friend — but they hit a physiological wall.
The executive ‘battery’ is not just flat, but broken due to chronic overuse (masking, sensory effort), and the body has pulled the emergency brake. Understanding that this inertia is a biological incapacity, and not a lack of willpower, is essential to breaking the cycle of guilt and shame.
———
Major Depression: A Clinical Perspective
Slide 05 / 18 Major Depression: Clinical Perspective Main features: anhedonia, hopelessness, apathy. Standard treatment is based on changing behaviour and thinking.
Clinical context To avoid misguided treatments, we must first understand what neurodivergent exhaustion is most often confused with: major depression. From a clinical perspective, depression is primarily characterised by anhedonia, that is, the inability to feel pleasure or interest in activities that once brought joy. The dominant feeling is one of hopelessness, apathy and a generalised negative outlook towards oneself and the world.
In depression, the central issue is often linked to motivation (“I don’t want to do this”) and a distorted view of reality. Standard treatments for depression are based on the idea that, by changing behaviour and thinking, one can change one’s emotional state. However, this definition does not fully capture the reality of a neurodivergent person whose nervous system has simply broken down due to a lack of resources, not a lack of interest.
———
Overlapping Symptoms
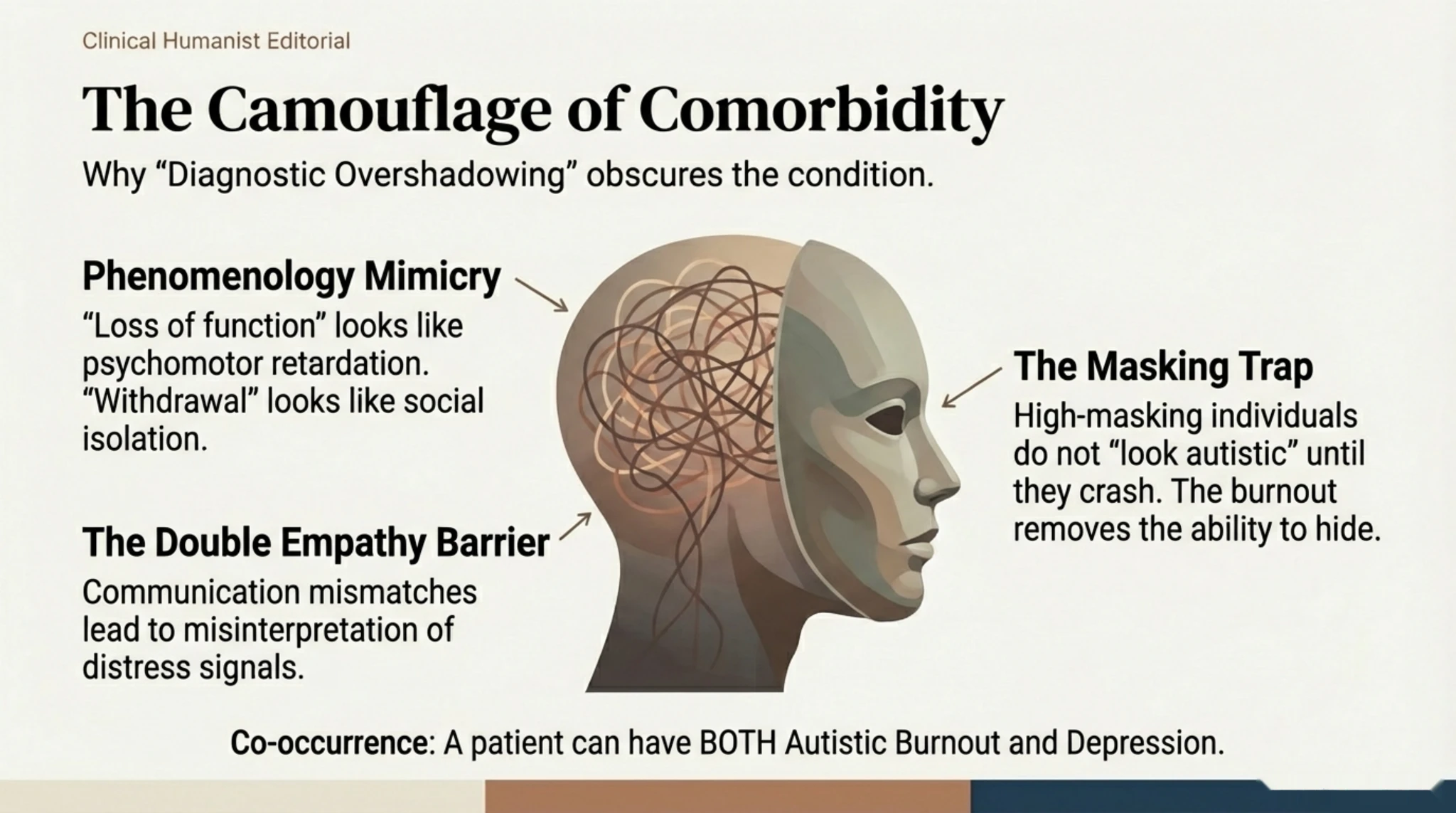
This Venn diagram visually illustrates why so many doctors and patients confuse the two conditions. There is a significant overlap in outward symptoms: both conditions manifest as extreme lethargy, social withdrawal, ‘brain fog’ (cognitive difficulties), executive dysfunction and sleep problems. From the outside, a person experiencing burnout looks almost identical to a person with depression.
However, the internal mechanisms are different. For example, a ‘flat affect’ (reduced expressiveness) in burnout may be a strategy for conserving energy (reduced masking), whereas in depression it reflects a lack of emotion. Understanding this overlap is vital to avoid drawing hasty conclusions based solely on observable behaviour, whilst ignoring the root cause: the depletion of resources.
Clinical Alert: Diagnostic Overlap
A recent study (Arnold et al., 2023; confirmed by Mantzalas et al., 2024) found that 98% of autistic people experiencing burnout meet the clinical criteria for a diagnosis of Major Depressive Disorder. However, the aetiology and treatment are completely different. In autistic burnout, social withdrawal is a coping mechanism, and engagement in special interests provides energy. In depression, social withdrawal is both a cause and a consequence of the illness, and the person loses pleasure (anhedonia) in their passions.
———
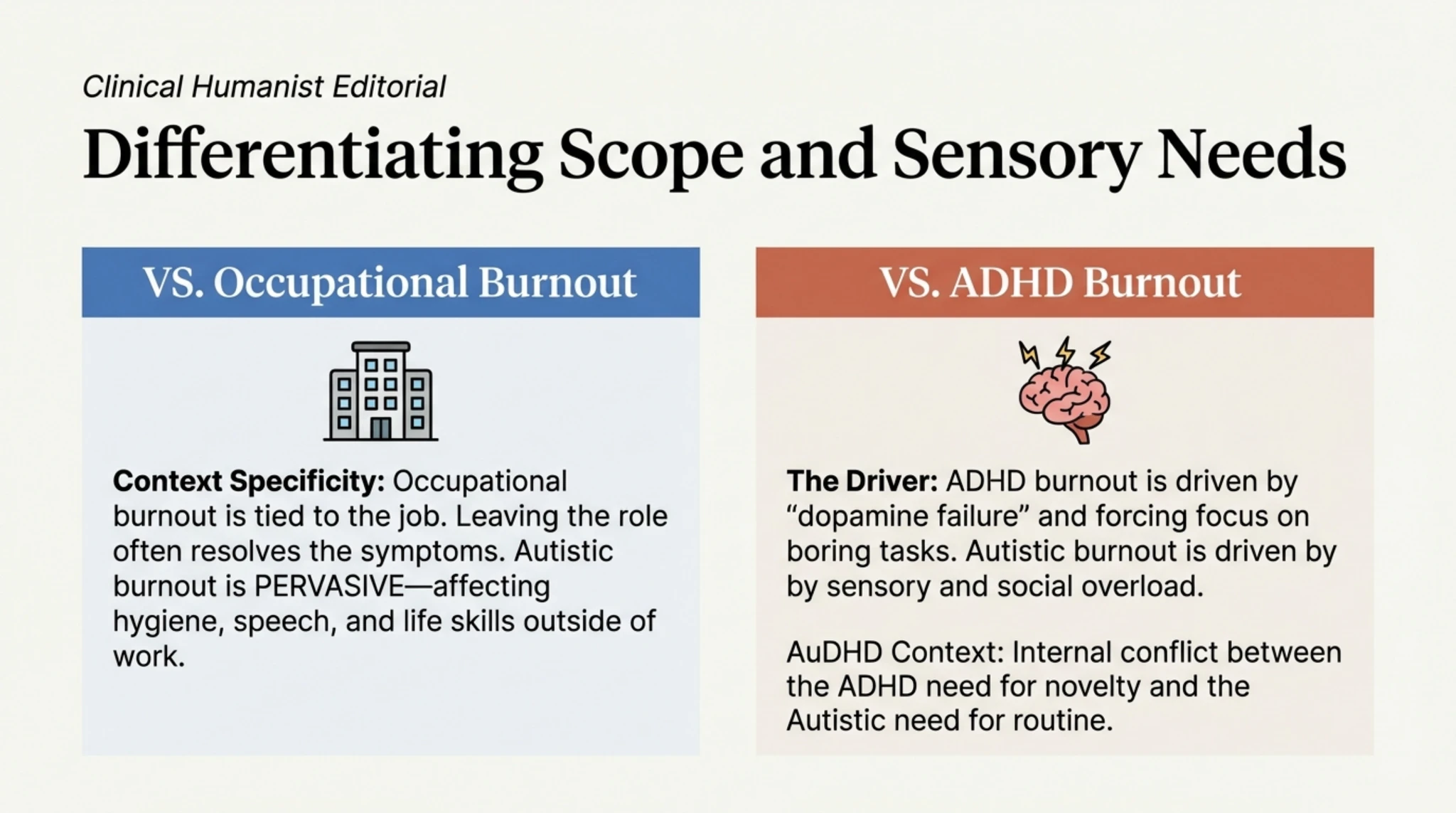
It is not just Depression
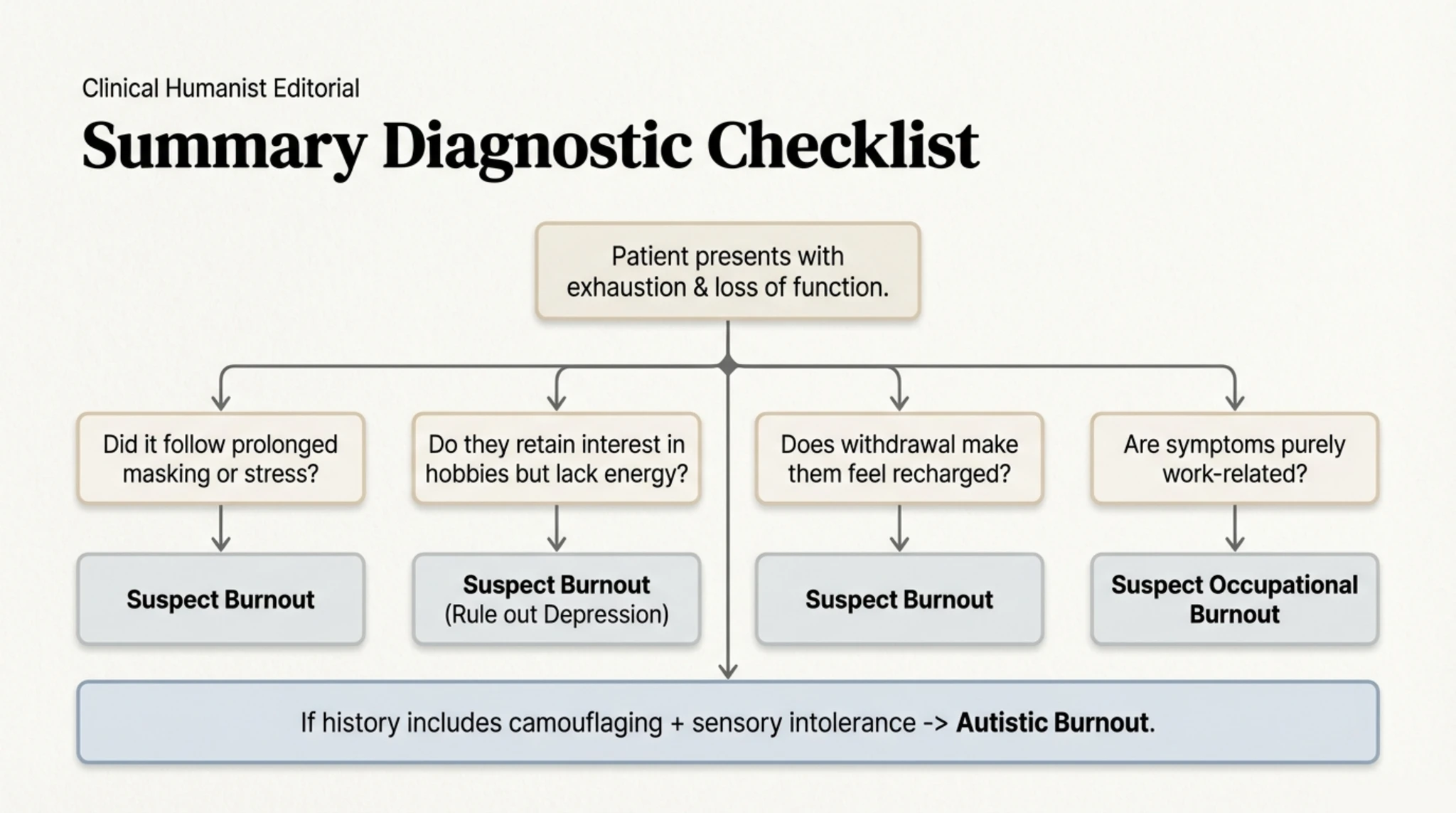
Here we make the critical distinction between “I want to, but I can’t” (specific to burnout) and “I don’t want to anymore” (specific to depression). In neurodivergent exhaustion, the person often wants to engage in their projects, but hits a physical and cognitive wall — a functional incapacity. In contrast, depression involves a loss of desire itself. This nuance radically changes the approach to the necessary treatment.
———
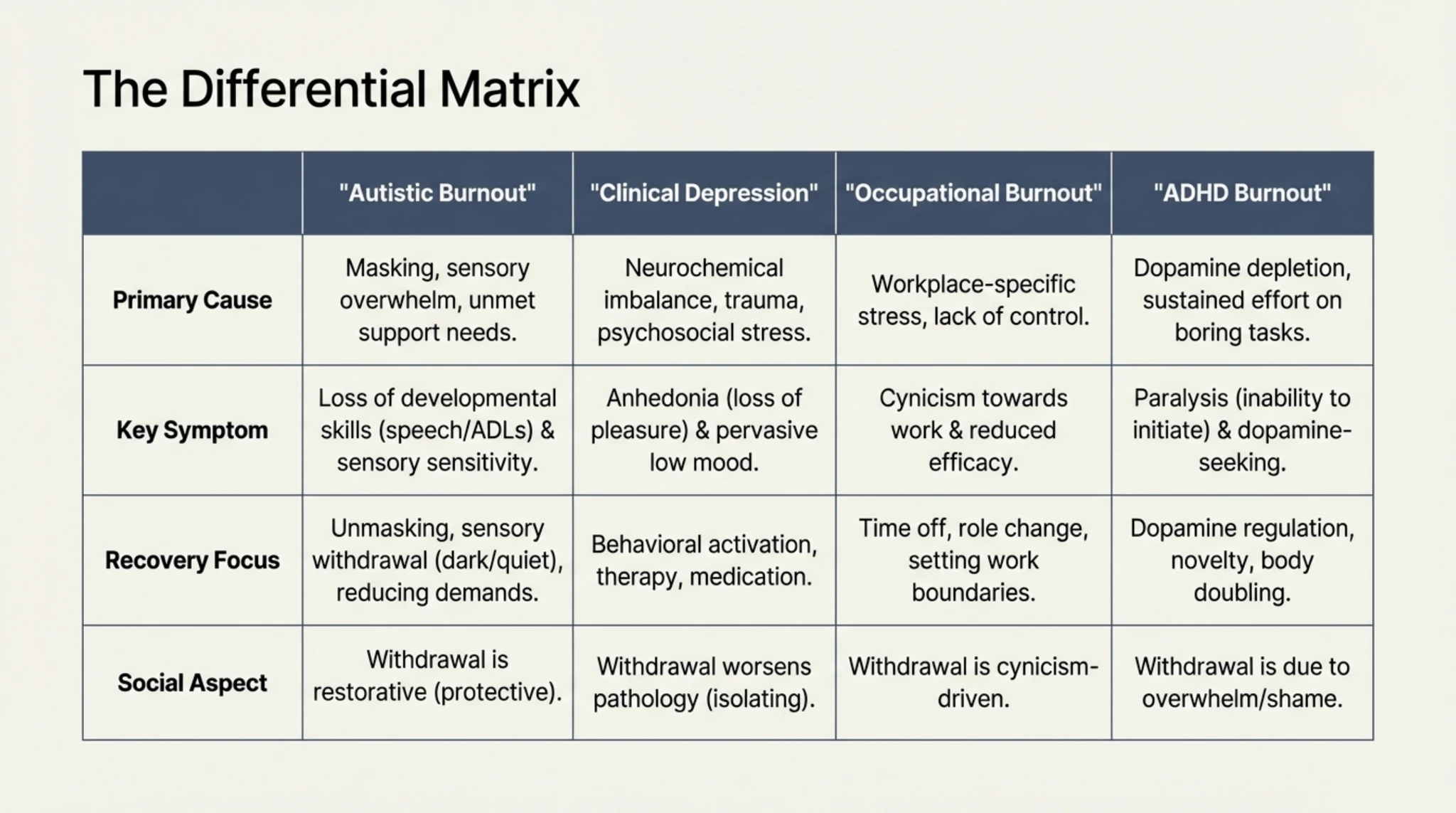
Comparative Table: Distinctive Signs
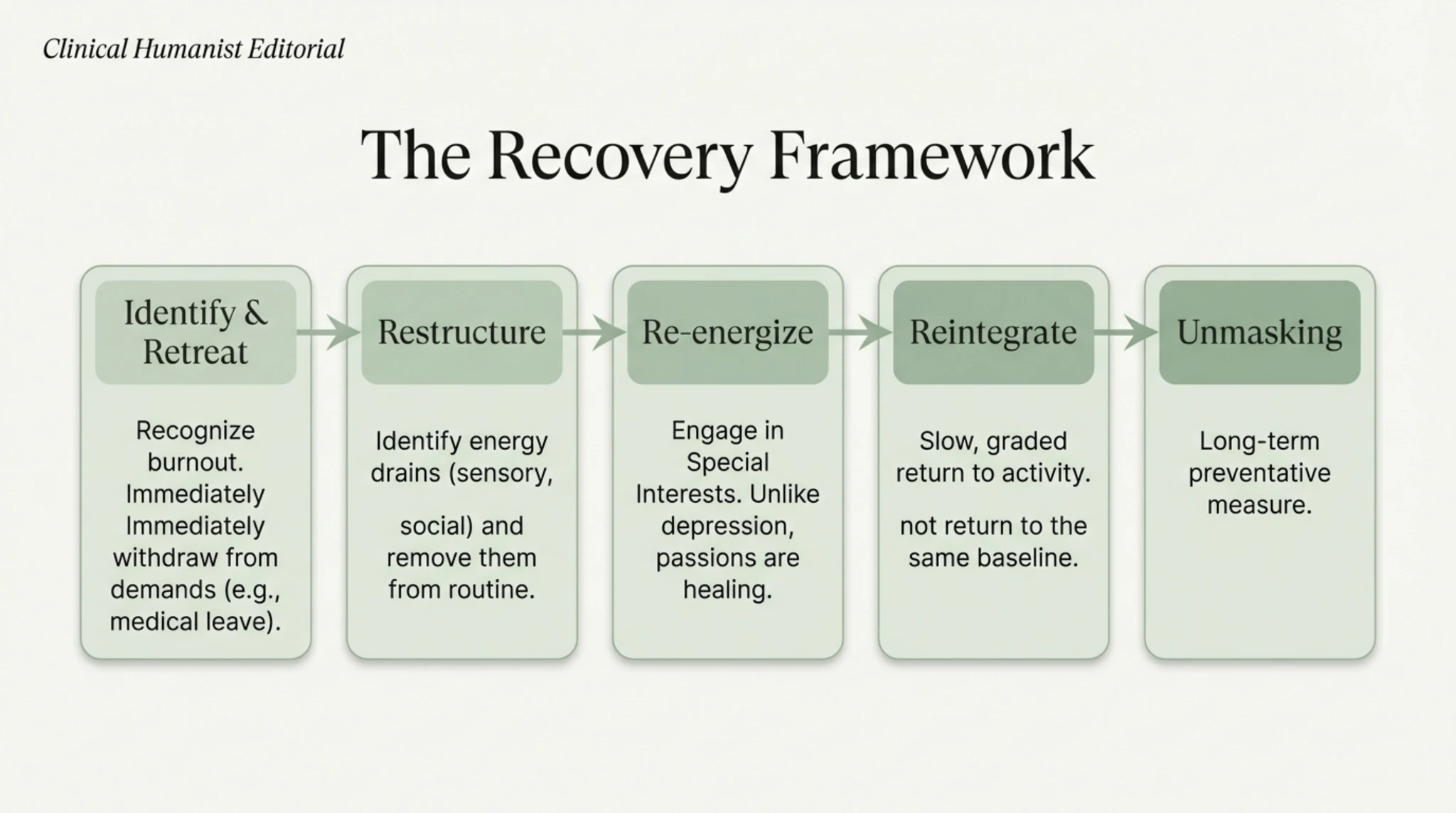
We analyse the qualitative differences in detail, focusing on the relationship with special interests and the response to rest. In an episode of burnout, special interests (intense passions) are still desired and can function as a source of regeneration, although the person may be too tired to actively pursue them. In depression, these interests lose their appeal entirely due to anhedonia.
Furthermore, the response to rest differs fundamentally. Neurodivergent exhaustion improves slowly through ‘radical rest’ and a reduction in sensory input, whereas depression does not usually respond to rest alone; indeed, isolation can even exacerbate it. Sensory sensitivity tends to increase acutely in burnout (everything hurts, lights are too bright), whereas in depression, sensory perception may be unchanged or even dulled.
———
Triggering Factors
It is important to recognise that untreated exhaustion is, in itself, a direct route to secondary depression. When a person loses their abilities, independence and capacity to function due to burnout, it is natural to develop feelings of worthlessness or despair, which lead to depression. Thus, burnout is the cause, and depression is the effect.
Other triggers specific to neurodiversity include isolation caused by a lack of authentic connection (the Double Empathy Problem) and the trauma of repeated invalidation. Understanding this causality helps us treat the source (burnout and lack of support) to alleviate depressive symptoms, rather than merely treating the symptoms without addressing the underlying energy deficit.
Recent research (published in the Interoception & Burnout journal) has demonstrated an additional mechanism: masking not only consumes energy — it actively suppresses interoception. To mask effectively, an autistic person must ignore internal signals of discomfort (suppressing stimming, forcing painful eye contact). Long-term practice of camouflage creates a psychological barrier between the individual and their own needs, turning the ignoring of pain and fatigue into an automatic response. This forced disconnection places immense pressure on the nervous system, inevitably leading to a breakdown of resources.
———
The Trap of Standard Treatment
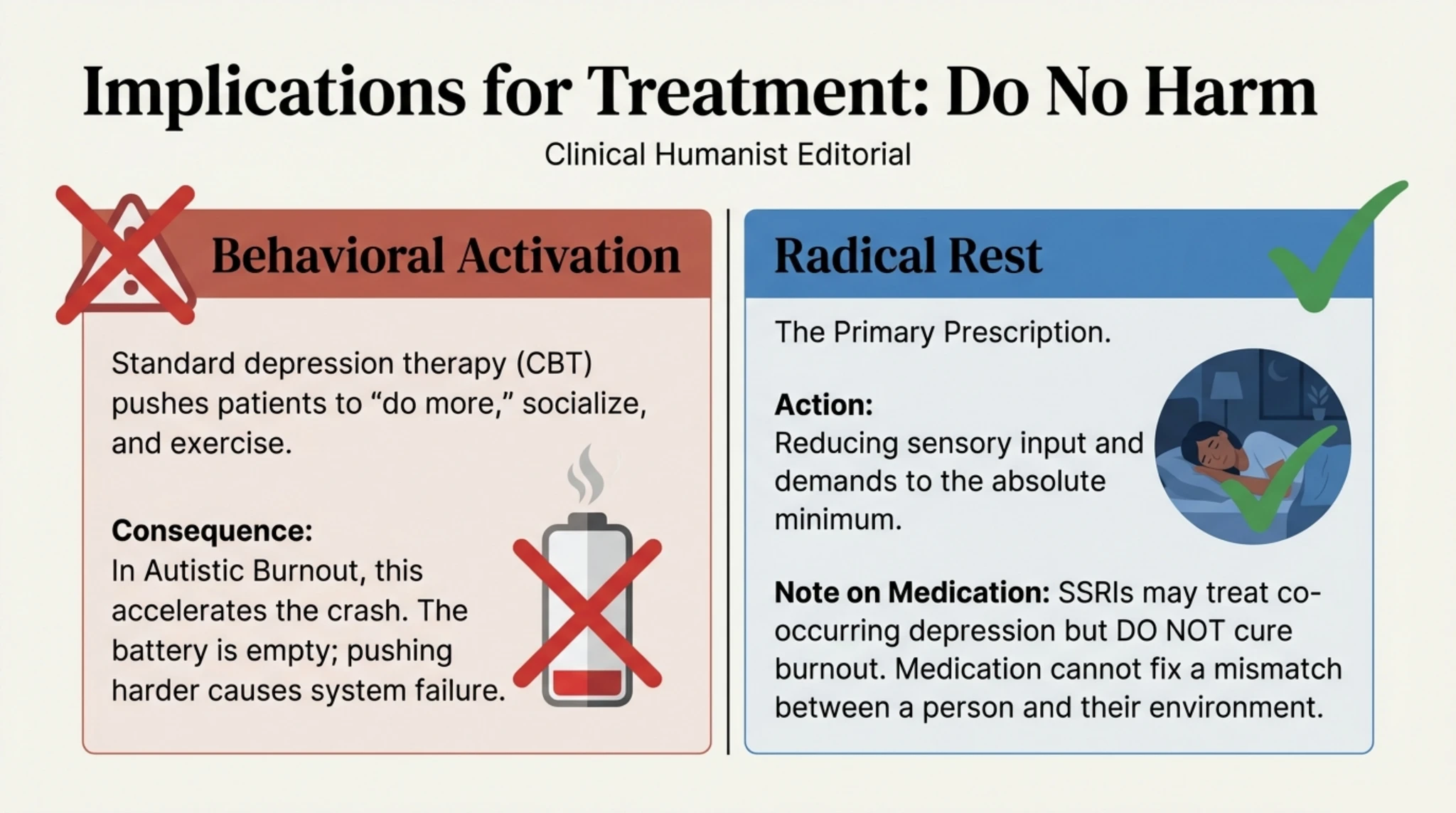
This diagram explains the mechanism by which well-intentioned therapies can do harm. In classic depression, the avoidance cycle is broken through action (‘fake it till you make it’), which can reactivate the reward circuits. However, for a neurodivergent brain in burnout, this approach is akin to driving a car without oil: the engine seizes up permanently.
Behavioural Activation, the standard treatment for depression that encourages the patient to be more active in order to improve their condition, can be disastrous in the case of burnout. Forcing an already exhausted nervous system to ‘get out more’ or ‘get some exercise’ will accelerate the collapse, deepening the crisis rather than resolving it. The correct solution is to reduce demands, not increase them.
Warning sign: risk of suicide
Research indicates alarming rates of suicidal ideation among autistic people experiencing burnout: 72% report suicidal ideation, of which 44% is directly associated with burnout. Autistic people are 25 times more likely to attempt suicide than non-autistic people. This statistic highlights the urgency of clinically recognising autistic burnout as a distinct entity from depression.
If you are in a crisis, contact the Lifeline: 0800 801 200 (free, 24/7)
———
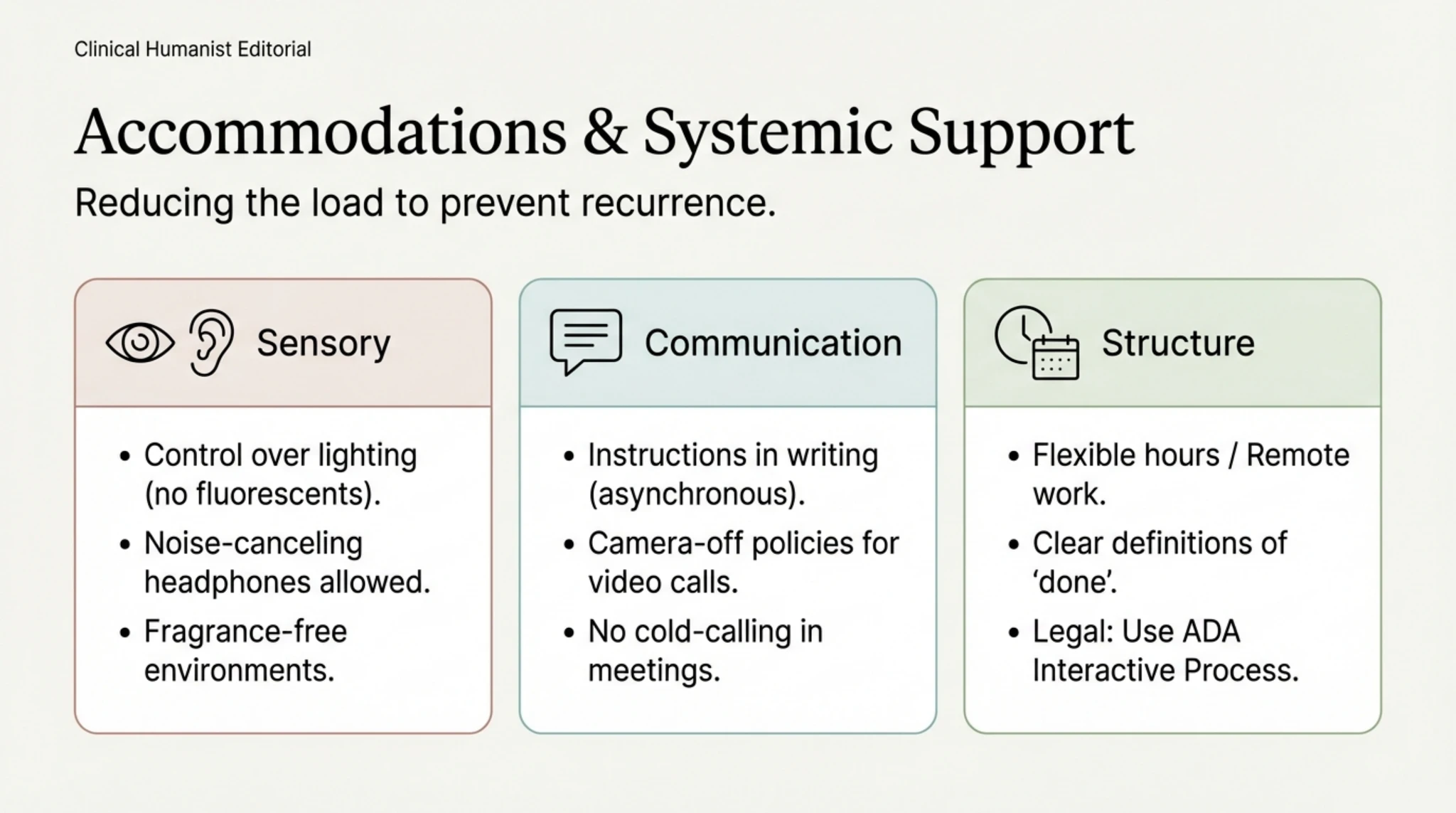
Do’s & Don’ts: A Neuroaffirmative Guide
Here is a clear visual guide to navigating recovery. In the ‘Don’t do this’ column, we have the depression model: pressure to socialise, intense physical exercise, and the cognitive reframing of limits as merely ‘negative attitudes’. These risk depleting the last of one’s resources and causing shame.
In the ‘Do this’ column (the Neuroaffirmative Model), we prioritise sensory rest, strategic solitude and validating limits as biological, not psychological. Using special interests as a form of therapy and adapting the environment are the right interventions. This clear distinction empowers the person to refuse unsuitable advice and protect their energy.
———
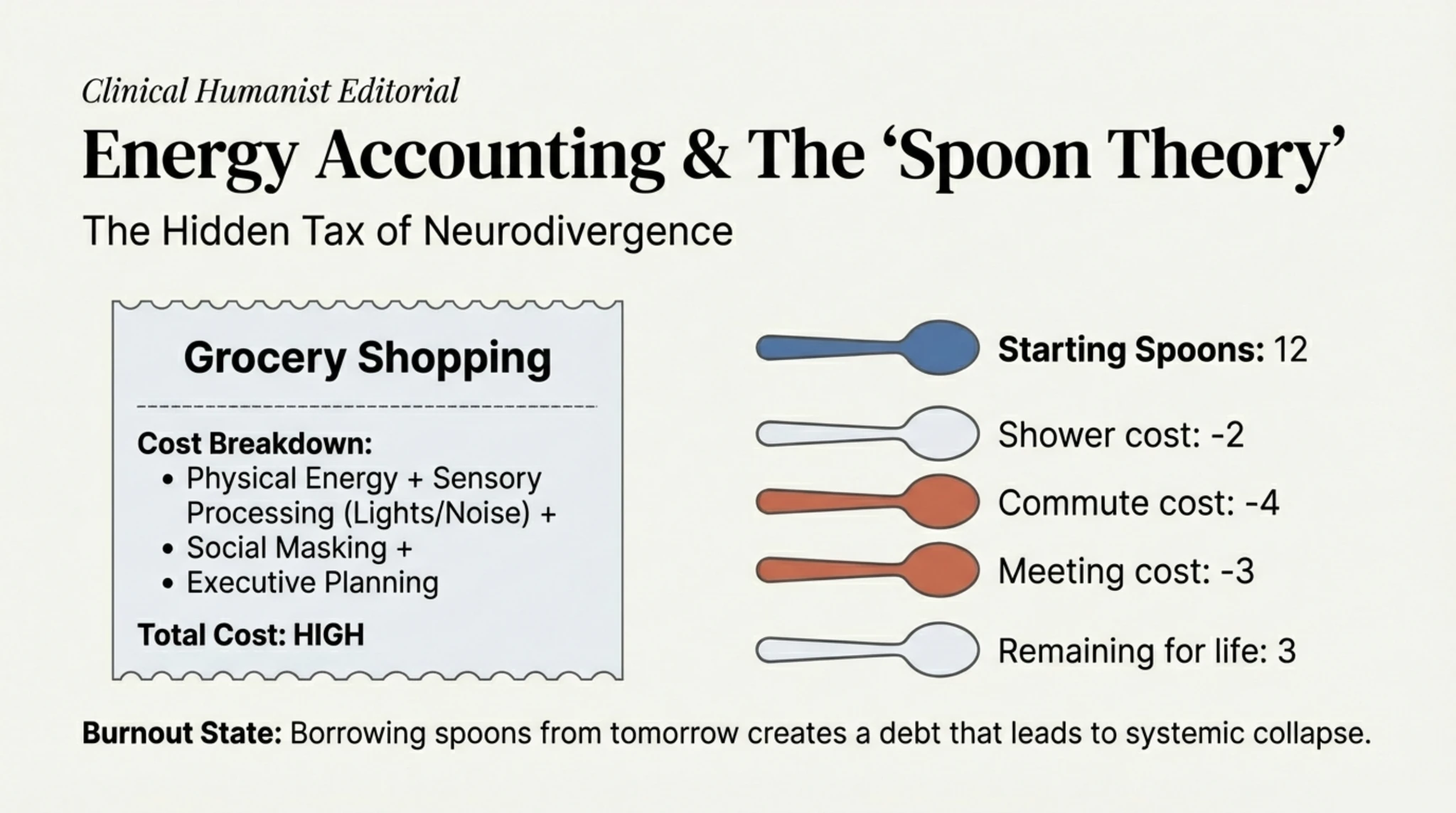
The Burnout Equation: What Drains Our Battery?
This slide visually introduces the energy equation of neurodivergent burnout. Every day brings a drain on resources from four simultaneous directions: behavioural masking, executive fatigue from constant planning and organisation, sensory overload, and minimising one’s own needs. When the sum of these demands consistently exceeds the capacity to recharge, burnout becomes inevitable — not a question of ‘if’, but of ‘when’.
———
The Burnout Equation: Why the Collapse Occurs
We move on to a logical explanation of the phenomenon through a simple formula: (High Stress + Lack of Coping Mechanisms + Masking) x Time = Burnout. This equation demonstrates that burnout is a mathematical result of resource consumption exceeding replenishment over a long period of time. The ‘Time’ factor is crucial, explaining why a person may seem to cope for years, until, suddenly, they can no longer do so.
This approach removes the stigma of ‘weakness of character’. It is not that the person is not strong enough, but that they have been operating in a state of chronic energy deficit. Executive fatigue, minimised needs and the cost of masking accumulate day by day, creating an energy debt that the body eventually demands be repaid.
———
The Drivers of Exhaustion: Why Does It Happen to Us?
Let’s break down the four main pillars that fuel the equation of exhaustion. Masking drains prefrontal resources to mimic neurotypical behaviour. Executive Fatigue stems from the constant effort to plan and organise in a chaotic world. Sensory Overload means continuously processing a hostile environment (lights, sounds) without breaks.
The fourth pillar, Minimised Needs, refers to internalised ableism — the tendency to ignore one’s own biological and sensory needs so as not to cause a disturbance or to appear ‘normal’. These four drivers operate simultaneously, draining the internal battery much faster than in neurotypical people.
———
The Invisible Cost of Masking
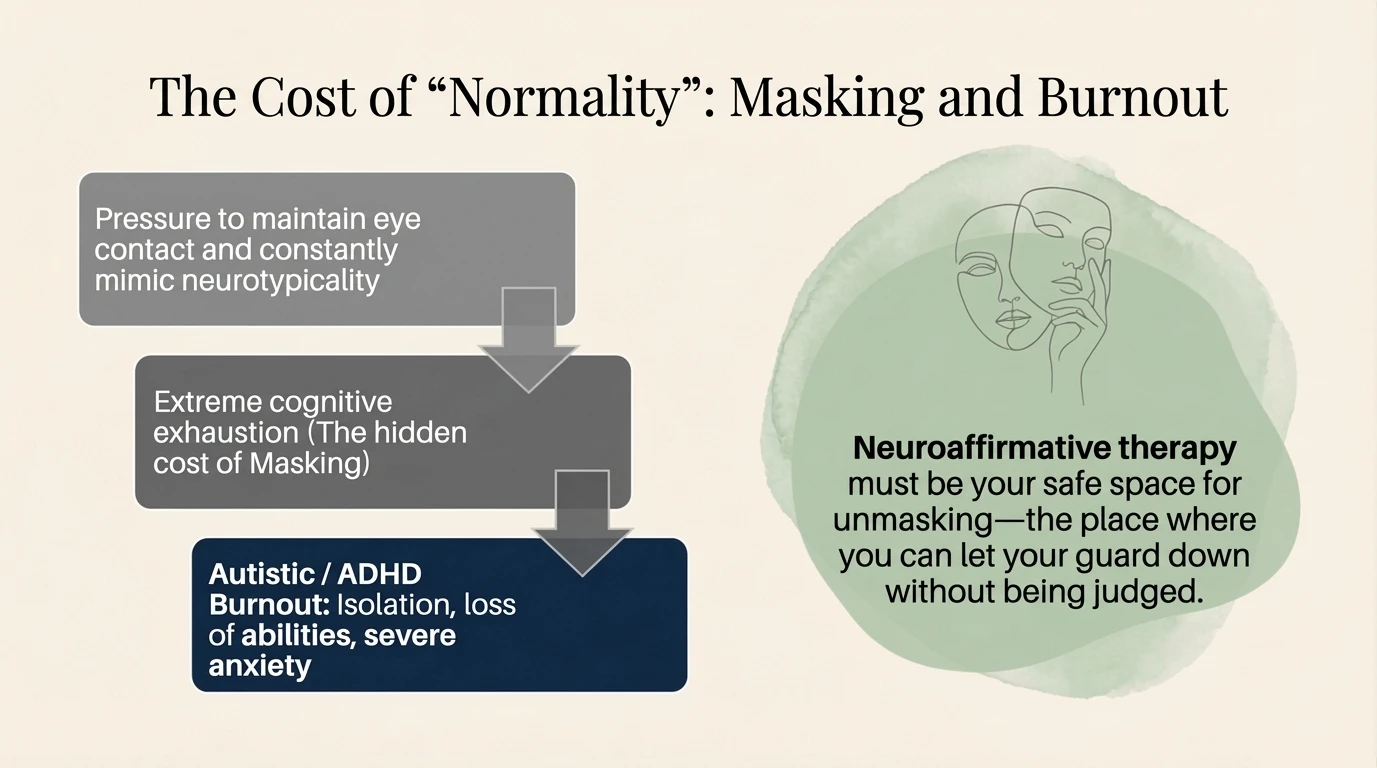
Masking is often the most energy-intensive process. Defined as the suppression of stimming (self-regulatory movements) and the forcing of eye contact, masking is a continuous performance. The ‘Psychic Plate’ metaphor suggests that masking leaves residues of stress which, over time, block the emotional ‘arteries’, leading to a disconnection from the self.
The effect of masking is twofold: it consumes massive amounts of cognitive energy and, simultaneously, blocks the nervous system’s natural regulatory mechanisms (such as stimming). The long-term solution for recovery involves not only rest, but also the creation of safe spaces where unmasking is possible and validated.
———
Why we don’t feel it coming: The Role of Interoception
Many neurodivergent people wonder why they didn’t stop before the breakdown. The answer lies in interoception, the ‘eighth sense’ that informs us of the body’s internal state. The diagram illustrates the three profiles: under-responsiveness (signals are ‘silent’), over-responsiveness (everything is felt too intensely, creating anxiety) and difficulties with discrimination (confusion between hunger, emotion or pain).
The impact is significant: if you do not feel your physiological limits, or if signals of fatigue are ignored or unclear, you will continue to work until you are completely exhausted. The body does not send gradual warnings, but seems to go straight from ‘fine’ to ‘collapse’, because the early signals were not consciously processed.
———
The Unseen Cause I: Interoception and the 3 Sensory Profiles
Interoception, often referred to as the ‘eighth sense’, is the system through which the brain receives information about the body’s internal state, such as hunger, thirst, heart rate and, crucially for burnout, available energy levels. For many neurodivergent people, the line of communication between the body and the brain works differently, which explains why exhaustion seems to strike suddenly, without the gradual warnings that neurotypical people experience.
If the brain does not receive the ‘notification’ that the internal battery has dropped to 20%, the person will continue to function at full capacity, ignoring biological needs, until the system shuts down forcibly through collapse.
This diagram details the three interoceptive profiles that contribute to this phenomenon of ‘blindness’ to one’s own state. Under-responsive (hyposensitive) people have their internal signals ‘muted’ and may forget to eat or not feel tired until the moment their body physically gives out.
Over-responsive (hypersensitive) individuals perceive any minor internal discomfort as a major emergency, living in a chronic state of alertness and anxiety that masks the specific signs of fatigue. Finally, those with difficulty distinguishing between sensations experience a vague and chaotic feeling of ‘being unwell’, but cannot pinpoint the exact source (confusing, for example, anxiety with hunger or emotional exhaustion with a physical illness), which prevents them from taking the right steps to rest in time.
———
The Unseen Cause II: Alexithymia vs. Autism
We conclude the first part by linking interoception to alexithymia — the difficulty in identifying and describing one’s own emotions. The diagram shows that, although alexithymia is common in autism, the two are distinct. The burnout mechanism is explained by the chain: Intense Physiological Reaction → Lack of Emotional Labelling (“I don’t know what I’m feeling”) → Continuing the Activity (“Pushing through”) → Physical Collapse.
This inability to name the state of overwhelm in a timely manner causes the person to miss the window of opportunity to take a preventative break. Thus, the breakdown seems to come out of the blue, but is in fact the result of unintentionally ignoring an accumulation of stress that the conscious mind could not put into words.
1. Autistic Burnout — Fundamental Research
- Raymaker, D. M., et al. (2020). “Having All of Your Internal Resources Exhausted Beyond Measure and Being Left with No Clean-Up Crew”: Defining Autistic Burnout. Autism in Adulthood, 2(2), 132–143.
- Mantzalas, J., Richdale, A. L., & Dissanayake, C. (2022). A conceptual model of risk and protective factors for autistic burnout. Autism Research, 15(11), 2013–2030.
- Higgins, J. M., et al. (2021). Defining autistic burnout through experts by lived experience: Grounded Delphi method investigating #AutisticBurnout. Autism, 25(8), 2356–2369.
- Arnold, S. R. C., et al. (2023). Towards the measurement of autistic burnout. Autism, 27(7), 1971–1987.
2. Alexithymia, Interoception and Emotions
- Shah, P., Hall, R., Catmur, C., & Bird, G. (2016). Alexithymia, not autism, is associated with impaired interoception. Cortex, 81, 215–220.
- Murphy, J., Catmur, C., & Bird, G. (2018). Alexithymia is associated with a multidomain, multidimensional failure of interoception. Journal of Experimental Psychology: General, 147(3), 398–408.
- Luminet, O., Bagby, R. M., & Taylor, G. J. (Eds.). (2018). Alexithymia: Advances in Research, Theory, and Clinical Practice. Cambridge University Press .
- Mahler, K. (2017). Interoception: The Eighth Sensory System. AAPC Publishing.
- Brewer, R., Cook, R., & Bird, G. (2016). Alexithymia: A general deficit of interoception. Royal Society Open Science, 3(10), 150664.
3. Masking (Social Camouflage)
- Hull, L., et al. (2017). “Putting on My Best Normal”: Social Camouflaging in Adults with Autism Spectrum Conditions. Journal of Autism and Developmental Disorders, 47(8), 2519–2534.
- Pearson, A., & Rose, K. (2021). A conceptual analysis of autistic masking: Understanding the narrative of stigma and the illusion of choice. Autism in Adulthood, 3(1), 52–60.
- Cook, J., et al. (2021). Camouflaging in autism: A systematic review. Clinical Psychology Review, 89, 102080.
4. Books and Clinical Resources
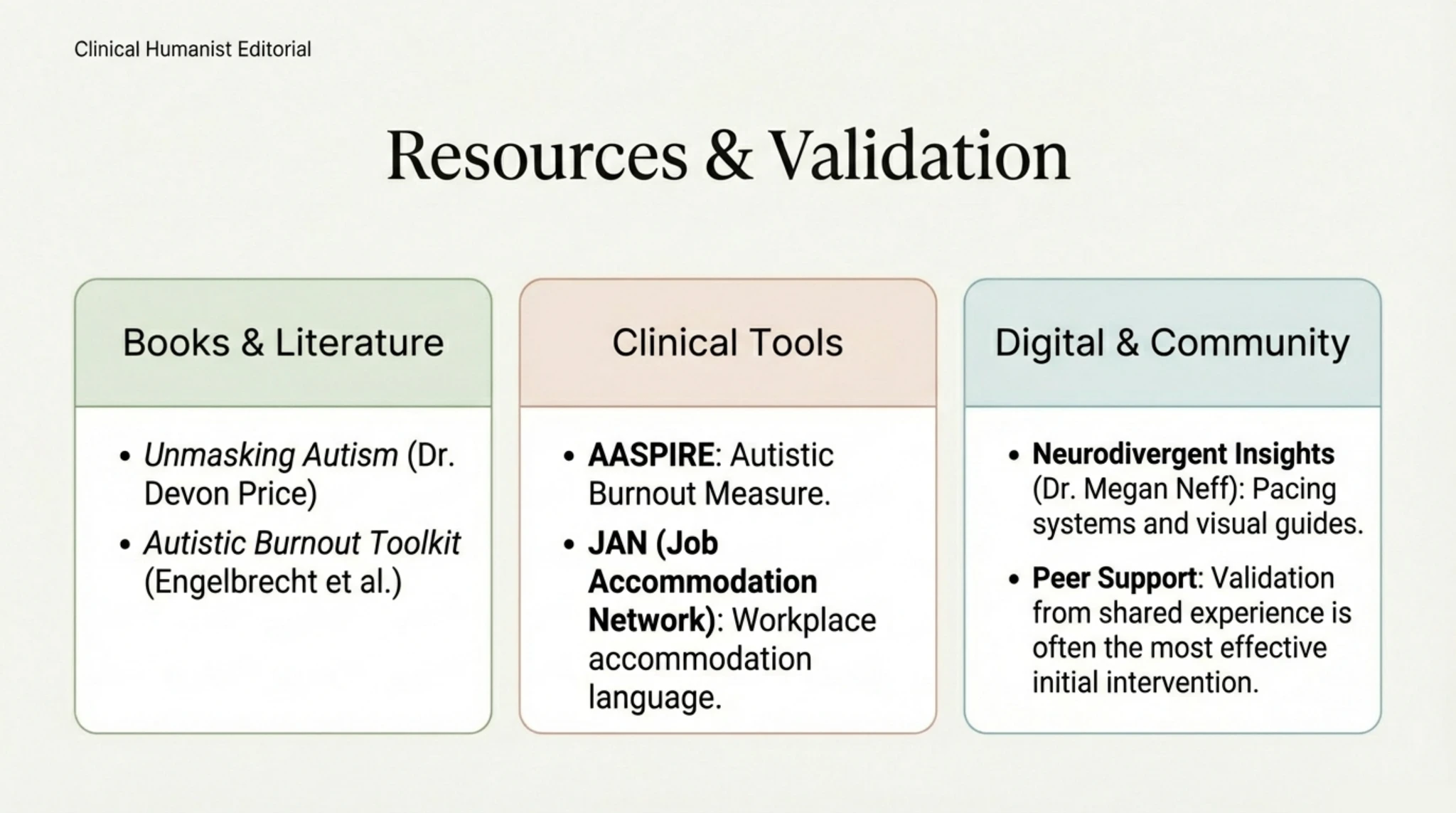
- Neff, M. A. The Autistic Burnout Workbook. New Harbinger Publications.
- Neff, M. A. Self-Care for Autistic People. New Harbinger Publications.
- Plumbly, C. (2025). The Trauma of Burnout: How to Manage Your Nervous System Before It Manages You. Balance.
- Engelbrecht, N., Bercovici, D., et al. The Ultimate Guide to Autistic Burnout. Embrace Autism.
5. Assessment Tools
- AASPIRE Autistic Burnout Measure (ABM) — Developed by the Raymaker/Arnold team.
- TAS-20 (20-Item Toronto Alexithymia Scale) — The gold standard for measuring alexithymia.
- CAT-Q (Camouflaging Autistic Traits Questionnaire) — For measuring the degree of camouflaging.
- MAIA (Multidimensional Assessment of Interoceptive Awareness) — For assessing interoception.
6. Recent Research (2023–2025)
- Mantzalas, J. et al. (2024). Autistic burnout: prevalence, risk factors and recovery. Autism Research.
- Ali, S. et al. (2025). Autistic burnout: A systematic review of 48 studies. Clinical Psychology Review.
- Bougoure, L. et al. (2025). Validation of the AASPIRE Autistic Burnout Measure (ABM). Autism.
- Arnold, S. et al. (2023). The overlap between autistic burnout and major depression. Autism in Adulthood.
Do these experiences sound familiar?
If you recognise yourself in what you’ve read, you’re not alone. Neurodivergent burnout is a real experience, validated by research, and there are neuroaffirmative strategies that can help.
Book an Initial Consultation → In Part 2, we will explore concrete strategies for recovery and prevention of neurodivergent burnout.
← Neuro-Affirmative Therapy (Part 2) The Anatomy of Burnout (Part 2) →

Next Steps
If this resonated, here are practical ways to go deeper.